Introduction
Exposure to herbicides during pregnancy has been linked to various adverse health outcomes in both the mother and the developing fetus (Rull, Ritz, and Shaw 2006; Parvez, Gerona, Proctor, et al., n.d.). Glyphosate is the active ingredient in many commonly used commercial and agriculture herbicides (Brantsaeter, Torjusen, Meltzer, et al. 2016). Significant animal and human research has suggested that herbicides cross the placenta and may increase the risk of certain diseases later in life, such as cancer and neurodevelopmental disorders (Baudry, Assmann, Touvier, et al. 2018; Carmichael et al. 2007; Rieg, Cattani, Naspolini, et al. 2022; Bradman et al. 2003; Bossi et al. 2013).
According to the Environmental Protection Agency, use of herbicides like glyphosate, has been significantly increasing in the United States (Benbrook 2016). Herbicides are widely applied to and absorbed by fruits, vegetables and wheat crops. As such, food intake is one potential route of human exposure (Ospina et al. 2022; Hood et al. 2022). Understanding how dietary consumption patterns correlates to biomonitoring herbicide concentration data is important as strategies are developed to reduce exposure (Connolly et al. 2017; Wei, Pan, Zhang, et al. 2024). However, there are few published data in pregnant cohorts regarding dietary consumption patterns and herbicides.
The objective of this analysis was to use dietary self-reported data in a United States Midwest pregnancy cohort to characterize patterns of food consumption in pregnancy. The hypothesis was that pregnant individuals would have dietary intakes that could be categorized into unhealthy and healthier eating patterns and additionally that the amount of organic food consumption could be incorporated. The ability to objectively classify individuals based on their self-reported dietary patterns could then be used to understand the contribution of diet to measured herbicide concentrations obtained during biomonitoring.
Methods
This study is an initial analysis of dietary intake patterns collected as part of the Heartland Study (HS). The HS is a multi-center observational pregnancy cohort which focuses on investigating the impact of herbicide exposure on adverse pregnancy outcomes. The HS is an ongoing study with planned recruitment of 2,000 pregnant individuals who are at least 18 years old and who are less than 21 weeks gestation. The full description of the HS is reported elsewhere (Freisthler et al. 2023). This analysis was planned as an exploration of how to best characterize the dietary intake patterns of an pregnancy group of HS participants.
Once 500 of the anticipated 2,000 participants were recruited, a planned analysis of the performance of the food frequency questionnaire was undertaken. The food frequency questionnaire was developed for this study to assist with capturing granularity of the types of food consumed and the percentage of the food that was organic. It was developed specifically for the HS since existing validated tools were not found that suited the overall HS aims (Freisthler et al. 2023). The full food frequency questionnaire is included in the Supplementary Appendix.
The study data were derived from two participant self-reported surveys following enrollment: a pregnancy preconception survey and the food frequency questionnaire. The pregnancy preconception survey, administered once after enrollment, collected socio-demographic factors. Factors included in this study included age, self-reported race and ethnicity, marital status, annual family income, financial assistance, geographical area of residence, number of individuals in the household, level of education completed, and tobacco and alcohol use.
The food questionnaire, which was administered during each trimester, asked about consumption of fourteen main food categories, including tree fruits, vegetables, berries, melons, beans, dairy products, etc. (Supplemental Appendix). Food categories were further divided into a total of 89 specific foods. Food frequencies included 1 or less, 2-4, 5-7, 8-10, 11-13, or 14 and more servings per week. Additionally, respondents were asked to indicate the percentage of each consumed food which was organic, categorized as 0-10%, 11-32%, 33-66%, 67-90%, or 90-100%. Participants who did not answer the questionnaires completely were excluded from this analysis. We used responses from the earliest food questionnaire completed.
Descriptive characteristics of the cohort were summarized with rates and means and standard deviations. A latent class analysis (LCA) approach was employed to analyze the cohort and responses related to the 89 foods from the fourteen food domains (Muthen and Muthen 2000; McCulloch et al. 2002; Morland and Filomena 2007). To determine the best number of classes for the LCA, we used the Bayesian Information Criterion (BIC) as the primary fit statistic (Drton and Plummer, n.d.; Neath and Cavanaugh 2012). This statistical method enabled the identification of distinct groups within the cohort based on their higher or lower consumption of foods including specific fruits, vegetables, grains, juices, sauces, and dairy foods, as well as the percentage of organic foods. For the purpose of this analysis, organic consumption levels below 10% were categorized as low, while consumption levels above 10% were considered “significant”. The sociodemographic differences were then compared between the groups. Statistical comparisons were performed using Chi-square tests for categorical variables and general linear models for continuous variables. All statistical analyses were performed using SAS, version 9.4 (SAS Institute, Cary, NC).
Results
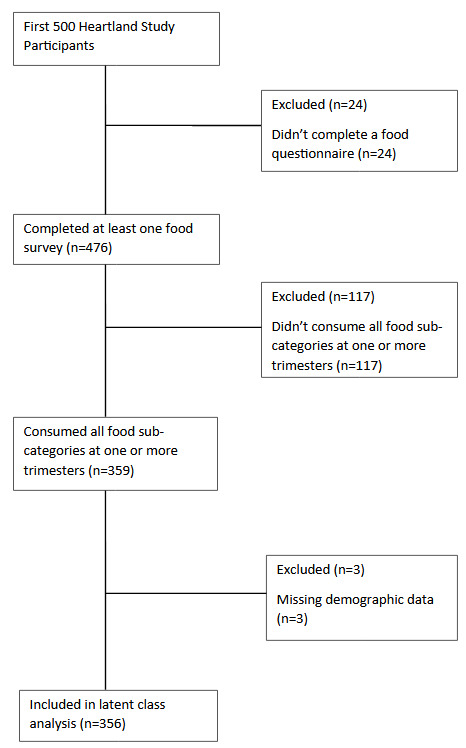
Of the first 500 participants recruited, 476 participants (95.2%) completed at least one food questionnaire survey. Our analysis was based on the 359 of those (75.4%) who reported consuming at least one of the foods at one or more trimesters.
The characteristics of the cohort are provided in Table 1. The average maternal age was 29.9 (±5.0) years. Additionally, the majority of participants in our cohort were Caucasian, were married, had completed a college education, and resided in suburban areas.
The overall responses regarding food groups consumed is in Table 2. Most participants reported consuming up to four servings of apples, oranges, and bananas per week, with very few consuming more than seven servings of tree fruits. Nearly two-thirds or more of the cohort who consumed tree fruits reported that 10% or less of the fruits they consumed were organic (Table 3). In general, for most food groups, consumption of organic foods was low in about 60-80% of individuals self-reporting (Table 3).
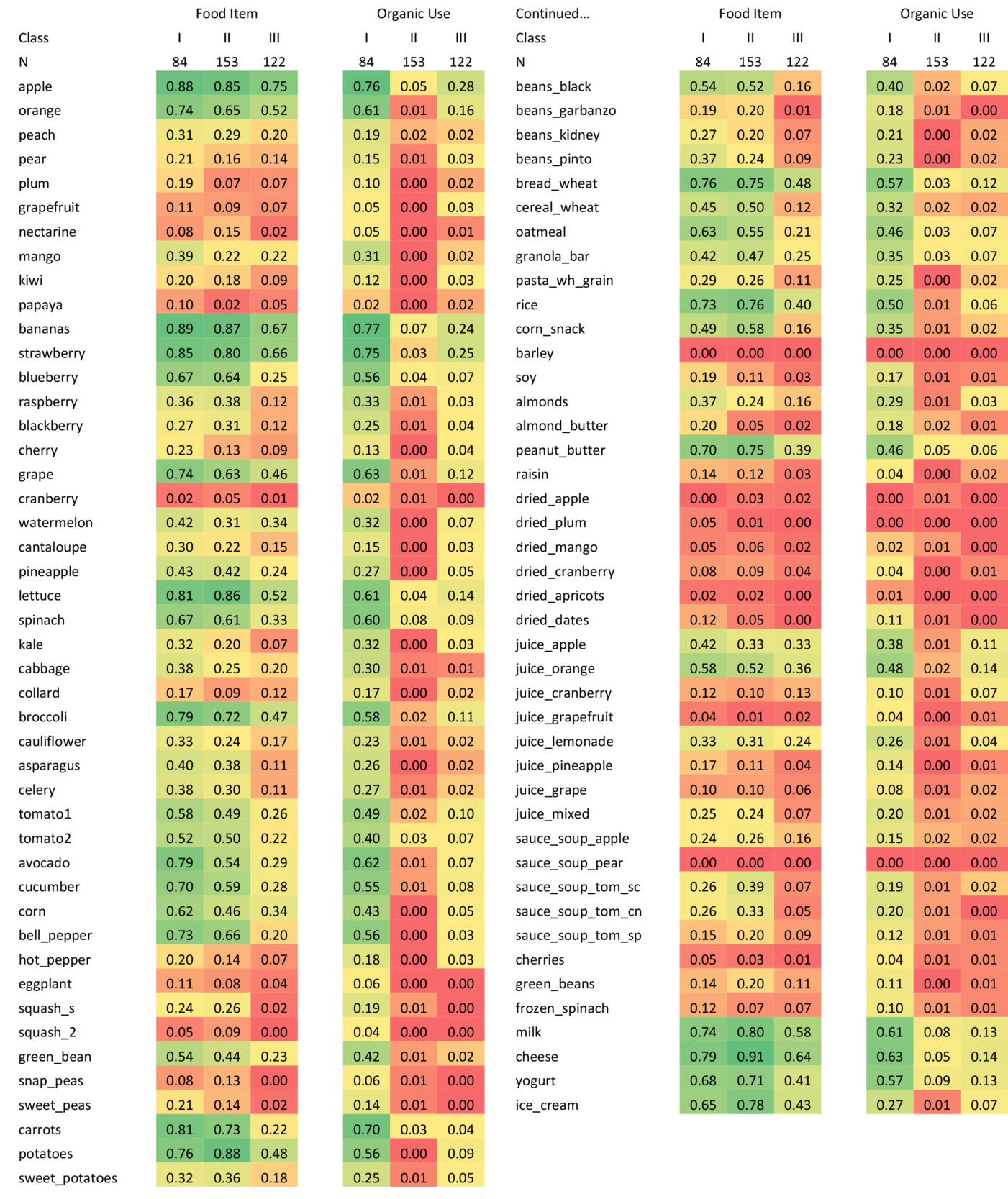
The best fitting LCA model revealed three distinct classes based on both the types of food and the percentage of organic foods consumed. To determine the number of classes for the LCA model, models were fit with two to five classes and goodness-of-fit criteria were used to select the final model. A three-class LCA model had the lowest (best) BIC (Supplementary Table). This resulted in three distinct classes defined by both food type and percentage of organic foods consumed. [Figure 2, Table 4] Class I represented a group who consumed a high amount of tree fruits, vegetables, berries, and other foods, with a high percentage of organic intake (n = 84, 23.4% of participants). This class was defined as the “healthy diet, higher organic” group. Class II (n=153, 42.6%) comprised those who consumed a high amount of the same types of healthy foods, but with a low percentage of organic intake. This class was defined to be the “healthy diet, lower organic” group. Class III (n=122, 34.0%) consisted of participants who consumed a low amount of tree fruits, vegetables, berries, and other types of foods including healthy foods, with a low percentage of organic intake. This class was defined to be the “less healthy diet” group.


Socio-demographic characteristics differed between the 3 classes derived from LCA (Table 4). Participants who self-identified as African American or Other were more likely than those identifying as Caucasian or Hispanic to be in Class III (50.0%, 44.0%, 27.8%, 31.3% respectively, p=0.003). There were significant differences in sociodemographic characteristics between the three latent classes of dietary intake in maternal age, marital status, education, income quartile, smoking, and alcohol consumption (Table 4). In general, healthier diets (Classes I and II combined versus Class III) were associated with self-reported Caucasian and Hispanic groups, older age, being married, having higher education, having a higher self-reported income quartile, and never smoking. Interestingly, 75.1% of individuals reporting current or recent alcohol consumption (within three months of pregnancy) were in Classes I and II, compared to 56.3% of former consumers and 55.3% of never consumers. Geography of participant residence did not differ significantly across classes. Socio-demographic variables differed most noticeably between Classes II and III. There were also some socio-demographic trends for those participants in Class I. Those in higher income quartiles seemed to less often be classified in Class I, while never smokers and those never consuming alcohol tended to be classified in Class I more frequently than those reporting differently about smoking and alcohol.
Discussion
In this Midwest US pregnancy cohort, self-reported dietary consumption was categorized as healthy in the majority of respondents, with 23.4% additionally being classified into a higher organic food consumption class. This is similar to a recent survey which reported that approximately 31% of US individuals regularly purchase organic food (U.S. Environmental Protection Agency 2015). In general, LCA was able to group the respondents into three distinct classes based on their self-reported dietary consumption. We further characterized the differences in sociodemographic characteristics between the classes. This approach to classification, using information from self-reported dietary consumption, may be useful in future analyses related to herbicide exposure and its contribution to adverse pregnancy outcomes.
Food that has been grown or produced without the use of synthetic fertilizers, pesticides, or genetically modified organisms (GMOs) is labelled as “organic”. Organic farming practices prioritize the use of natural resources, such as compost and crop rotation, to maintain soil health and protect the environment (McCulloch et al. 2002). These foods are often perceived as being healthier, safer, and more sustainable than conventionally grown foods. The dollars spent on organic food has risen in recent years (Statista Research Department 2024). Organic food consumption patterns in pregnancy have gained significant attention in recent years (American College of Obstetricians and Gynecologists 2022). Pregnant individuals are often advised to pay close attention to their diet as it plays a significant role in both maternal and fetal health conditions and pregnancy outcomes (Rull, Ritz, and Shaw 2006; Arbuckle, Lin, and Mery 2001; Gerona, Reiter, Zakharevich, et al. 2022).
During pregnancy, the nutritional needs of the mother and developing fetus are altered. Eating a well-balanced diet that includes a variety of fruits, vegetables, whole grains, lean proteins, and healthy fats is essential for both maternal and fetal health. Organic foods might be able to offer additional benefits by providing higher levels of nutrients such as antioxidants, vitamins, and minerals (Barański, Srednicka-Tober, Volakakis, et al. 2014). Additionally, consuming organic foods may help reduce exposure to harmful chemicals and pesticides that have been linked to adverse health outcomes, including birth defects, developmental delays, and cancer (Curl et al. 2019; Liu, Curl, Brantsaeter, et al. 2023; Torjusen, Brantsaeter, Haugen, et al. 2014; Hyland, Spivak, Sheppard, et al. 2023).
Organic food consumption patterns during pregnancy vary by geographic location, cultural background, and socioeconomic status (Morland and Filomena 2007; Wang et al. 2020). In developed regions, such as the US and Europe, organic foods are more widely available and affordable than in developing countries. Studies have shown that socioeconomic status can play a significant role in organic food and nutritious food consumption patterns (Deshmukh-Taskar et al. 2007; Eikenberry and Smith 2004; Konttinen et al. 2013). Pregnant individuals from lower-income households may not have access to organic foods or may not be able to afford them. Our study demonstrated this as well, in which many participants with lower status on several socioeconomic factors were prevalent in Class III based on their self-reported dietary intake. This type of food insecurity, inability to access healthy foods, may contribute to pregnancy healthcare disparities (Kumar et al. 2011; UNICEF 2023).
Organic food consumption during pregnancy is a complex issue, and the studies examining it show some inconsistencies. While some studies have shown that organic food consumption during pregnancy is associated with better nutritional status, others have shown no significant differences (Vigar et al., n.d.). However, there have been multiple studies that showed that glyphosate exposure may lead to adverse pregnancy outcomes, such as preterm-birth, smaller newborns, and congenital anomalies (Rull, Ritz, and Shaw 2006; Parvez, Gerona, Proctor, et al., n.d.; Brantsaeter, Torjusen, Meltzer, et al. 2016; Rieg, Cattani, Naspolini, et al. 2022; Gerona, Reiter, Zakharevich, et al. 2022).
Our study also noted disparities in self-reported race and ethnicity in the healthy food consumption classes. This is consistent with other studies which have noted the contribution of social determinants of health on healthy eating. For instance, a study in New York noted the absence of supermarkets in areas predominantly inhabited by black communities (Metoyer, Chuang, Lee, et al. 2022). The accessibility of grocery stores or supermarkets selling organic food to minority racial groups has been a subject of study. Some studies have indicated that African American and Hispanic populations face challenges in accessing stores with organic food, while others have reported the opposite. Additionally, some studies have focused more on the convenience of shopping rather than the proximity and distance of these stores (Kumar et al. 2011; D’Angelo et al. 2011; Di Noia et al. 2016; Evans, Banks, Jennings, et al. 2015; Sanchez-Flack et al. 2019; Zenk, Schulz, Hollis-Neely, et al. 2005).
Higher consumption of healthy foods and organic foods has been linked to older age groups, something also seen in our study (Simoes-Wust et al. 2017; Skreden et al. 2017). Higher educational attainment being associated with healthier dietary consumption in our cohort is also consistent with other studies (Wang et al. 2020; Simoes-Wust et al. 2017; Skreden et al. 2017; Kamphuis, de Bekker-Grob, and van Lenthe 2015).
Interestingly, in our analysis, a greater percentage of participants from suburban and urban areas were in Class I than were those who lived in rural areas. This may have been due to a lack of clarity about organic food on the survey, or that food in more urban areas is clearly marked as “organic” compared to rural areas. This bears future exploration.
Previous research has shown that the levels of biomarkers of pesticides in blood can be influenced by the type of foods that are consumed. Specifically, studies have observed that levels of urinary herbicides tend to decrease when individuals consume organic foods, and then increase again when they consume conventional or non-organic foods (Bradman, Quiros-Alcala, Castorina, et al. 2015; Lu et al. 2006). As the HS study continues, we will analyze the association between the dietary classes and urine herbicide concentrations. If confirmed, this could represent a potential therapeutic clinical recommendation that could be tested prospectively to reduce ingested chemicals and ultimately improve pregnancy outcomes.
This study has some limitations. The population was from a single area in the Midwest US, limiting generalizability. Additionally, while we were able to separate the cohort into three clear classes in this planned preliminary analysis, the class structure (number of classes; and food profile of classes) may need to be revised when the full cohort is analyzed. Additionally, the food frequency questionnaire utilized in the study was not validated, although it contains similar questions and response formats found on validated food questionnaires (Block et al. 1994; NIH Epidemiology and Genomics Research Program 2022). As our study was focused on herbicides, the food questionnaire did not include specific questions regarding meat consumption, which limited our ability to determine the impact of vegetarianism and may have led to underestimation of organic food consumption among individuals who predominantly consume meat-based diets. Also, the survey did not calculate calorie intake, macronutrient composition, and micronutrient content. Although we did not include body mass index that in the current analysis, we plan to explore its association with dietary choices, herbicide concentrations, and pregnancy outcomes in the full cohort. For those completing the survey during the first trimester, we did not capture the impact of nausea and vomiting of pregnancy. Several of these factors will be accounted for when the full cohort of 2,000 participants is analyzed in conjunction with the urine herbicide concentrations and pregnancy outcomes.
In conclusion, a latent class analysis was able to classify participants in a Midwest US pregnancy cohort into three classes based on self-reported dietary intake and organic food consumption. These groupings were highly associated with sociodemographic characteristics, highlighting the potential impact of social determinants of health on dietary choices available to and made by pregnant individuals. This type of grouping can aid in analyses of pregnancy outcomes and herbicide biomarker analysis and may yield information important to developing interventions to optimize pregnancy outcomes in the face of herbicide chemical exposures.
Conflict of Interest
The authors declare no financial conflicts of interest.
Funding
Funding for the Heartland Study is provided by the Heartland Health Research Alliance, a non-profit foundation. The funding agency had no role in the analysis or writing of this manuscript.