INTRODUCTION
Uterine lipoleiomyomas are benign neoplasms that are not often seen in clinical practice. First described in 1965, these entities were recognized by a composition of intermixed smooth muscle, mature adipocytes, and fibrous tissue (Manjunatha, Ramaswamy, et al. 2010; Johari, Koshy, et al. 2014). The incidence of lipoleiomyoma has always been accepted as 0.03-0.2% by Willen et al. in 1978 (Yuan, Chen, et al. 2021; Johari, Koshy, et al. 2014). However, recent studies propose a higher incidence at 2.9%, such as Akbulut et al. in 2014. Most commonly found in the uterus, these neoplasms can rarely be associated with the cervix, broad ligament, peritoneum, ovary, as well as other extrapelvic locations (abdominal wall, inguinal canal, vulva, and lung). These benign tumors present similarly to uterine leiomyomas in peri- and post-menopausal women with obesity, with symptoms of pelvic/abdominal pain, mild abnormal vaginal bleeding, constipation, increased urinary frequency, and possibly a palpable mass. We report two separate cases of uterine lipoleiomyoma seen at our institution from presentation, clinical management, and ultimately pathologic diagnosis.
CASE REPORTS
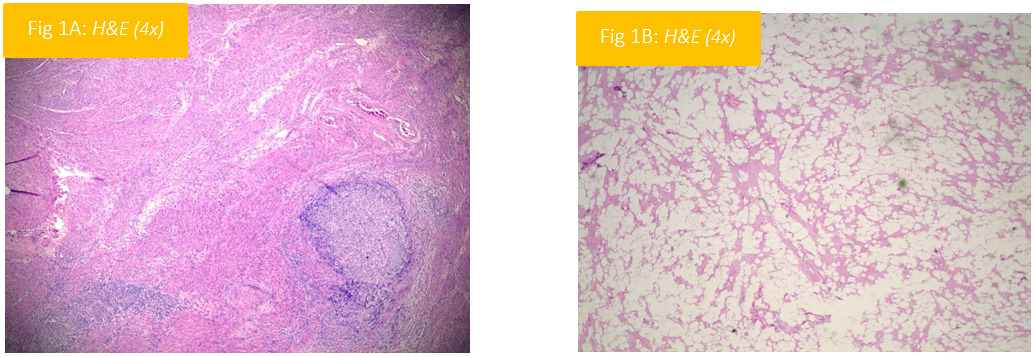
A 51-year-old female presented with six months of severe post-menopausal bleeding, severe left-lower quadrant pelvic pain, and lightheadedness. Gynecologic/obstetric history was as follows: gravida 3, para 2, no history of abnormal cervical cancer screening, and no supplemental hormone use. The patient reported no personal or family history of gynecologic or breast cancer. Of note, patient’s body-mass index (BMI) was 30.2, and she had a 50 pack-year smoking history. On physical exam, there were no identifiable abnormalities of the external genitalia, vagina, or cervix. No palpable masses were appreciated on bimanual exam, nor did the patient report pain on exam. Transvaginal ultrasound revealed a heterogeneous, thickened endometrium of 3.9 centimeters and a probable left ovarian dermoid cyst. Computed tomography (CT) showed distension of endometrial cavity due to polyps and/or submucosal masses, as well as a fat-containing mass in the uterine corpus. Hysteroscopy with dilation and curettage was performed with pathology of high-grade malignancy. Differential diagnosis at this time included high-grade stromal sarcoma, undifferentiated carcinoma, adenosarcoma, or malignant mixed Mullerian tumor. Patient underwent magnetic resonance imaging (MRI) due to concern for malignancy, which showed FDG-avid endometrial thickening with no other FDG-avid areas of concern. Surgical treatment included a robot-assisted total laparoscopic hysterectomy, bilateral salpingoophrectomy, sentinel lymph node mapping, and pelvic/peri-aortic lymph node dissection without complication. Histopathologic diagnosis found carcinosarcoma of the uterus, two positive lymph nodes, and an incidental finding of lipoleiomyoma (see figure 1A and 1B). Further medical management will include chemotherapy and vaginal cuff brachytherapy for uterine carcinosarcoma.

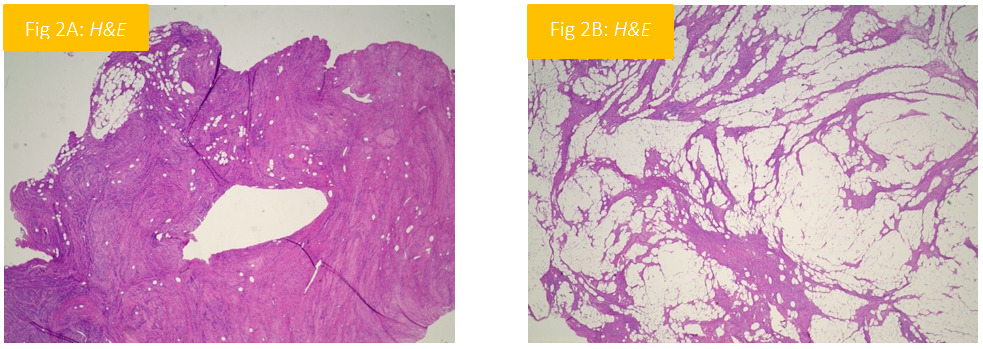
A 50-year-old female presented with increasing vaginal spotting and worsening urge incontinence. Gynecologic/obstetric history was as follows: uterine fibroid(s), gravida 5, para 5, no history of abnormal cervical cancer screening, current Mirena intrauterine device. The patient reported no personal or family history of gynecologic or breast cancer. Of note, patient’s body-mass index (BMI) was 32.7, and she had previously undergone bariatric surgery. On physical exam, there were no identifiable abnormalities of the external genitalia or vagina. The cervix was poorly visualized due to posterior fornix mass. The patient did not report pain on exam. Computed tomography (CT) showed increased size of heterogeneous mass in right lateral uterine wall, consistent with previously identified fibroid/leiomyoma. An adjacent fat-containing lesion was identified within the uterine wall. Patient underwent magnetic resonance imaging (MRI), which revealed large uterine mass at fundus with associated fatty component. Due to abnormal rate of growth of fibroid and fat component, there was concern for uterine sarcoma and/or malignant transformation of leiomyoma. Surgical treatment included a robot-assisted total laparoscopic hysterectomy, bilateral salpingectomy, and right oophorectomy for right ovarian cyst grossly identified at time of operation without complication. Histopathologic diagnosis found diffuse smooth muscle with increased cellularity and without mitotic nuclei or nuclear atypia interspersed with variable densities of adipocytes consistent with lipoleiomyoma with benign atrophic endometrium, paratubal cysts of bilateral fallopian tubes, and follicular cyst of the right ovary. No other management was indicated at this time, and follow-up in one year was recommended.

Pathogenesis
The pathogenesis of uterine lipoleiomyomas is somewhat perplexing since the uterus inherently contains no adipose tissue. Historically, there were many hypotheses explaining the origin of adipocytes, such as surgical deposition of adipose tissue into the myometrium, migration of adipocytes from peritoneal or retroperitoneal fat, as well as others. Currently, it is accepted that the origin of these adipocytes is multifactorial. One accepted theory hypothesizes the lipomatous component arises from direct transformation of totipotent mesenchymal cells in response to changes within the microenvironment of the tissue (Yuan, Chen, et al. 2021; Manjunatha, Ramaswamy, et al. 2010; Wilke, Benson, et al. 2022). These stressors include hypoxia and serum starvation, due to poor vascular availability within these lesions. Ono et al. isolated populations of myometrial cells with progenitor properties that could respond to hypoxic conditions by differentiating into myocytes and adipocytes. Studies have shown higher expression of hypoxia-inducible factor 1-alpha (HIF-1a) in avascular areas of uterine leiomyomas compared to healthy myometrium, suggesting a degree hypoxia and nutrient deprivation of the leiomyoma compared to healthy tissue that could transform mesenchymal cells into adipocytes. This transformation of progenitor cells and proliferation of the fibroid may be controlled by the Wnt signaling pathway via an “adipogenic switch”. In 2005, Arango et al. described differentiation of uterine myocytes to adipocytes in response to beta-catenin/Wnt signaling pathway suppression (Yuan, Chen, et al. 2021).
Other studies found chromosomal abnormalities, such as t(5;12) and t(12;14), present in lipoleiomyomas. Chromosomal rearrangements involving the long arm of chromosome 12 have been described in traditional leiomyomas, as well as lipomas. There is speculation whether these chromosomal translocations of traditional leiomyomas, lipoleiomyomas, and lipomas are related, due to the paucity of chromosomal studies due to formalin fixation of tissue (Yuan, Chen, et al. 2021).
There is also an effect of estrogen levels on leiomyoma cell proliferation (Manjunatha, Ramaswamy, et al. 2010). Although most leiomyomas typically decrease in size after menopause due to insufficient estrogen and decreased levels of sex hormone-binding globulin, the bioavailability of estrogen increased post-menopause which may contribute to lesion growth (Yuan, Chen, et al. 2021). Estrogen therapy is widely-used for management of menopausal symptoms, and this degree of long-term estrogen exposure may be a factor in lesion growth or lipoleiomyoma formation through secreted frizzled-related protein 1 (SFRP1) which inhibits WNT/beta-catenin signaling (Yuan, Chen, et al. 2021). Hyper-estrogen states have been associated with lipoleiomyoma occurance, such as endometrial hyperplasia, polyps, endometriosis, adenomyosis, and gynecologic cancers (Yuan, Chen, et al. 2021; Wilke, Benson, et al. 2022). Associated metabolic disorders with hyperestrogenic states have also been shown to play a role in the development of lipoleiomyomas. Such conditions may include obesity, hyperlipidemia, hypothyroidism, hypertension, and diabetes mellitus (Yuan, Chen, et al. 2021; Manjunatha, Ramaswamy, et al. 2010; Wilke, Benson, et al. 2022). Although an association between metabolic disorders and hyperestrogenic states have been seen in patients with lipoleiomyoma, there have been cases where no metabolic disorder was found. Nevertheless, prompt screening for metabolic disorders, hyperestrogen etiology, or gynecologic malignancy is warranted when a suspected leiomyoma has a lipomatous component.
PRESENTATION
Lipoleiomyomas typically occur in peri- or post-menopausal women with obesity. Although most are asymptomatic, some patients will present with symptoms similar to that of an uterine leiomyoma: abnormal uterine bleeding, pelvic/abdominal pain, constipation, urinary incontinence, and/or a palpable mass (Yuan, Chen, et al. 2021; Manjunatha, Ramaswamy, et al. 2010; Wilke, Benson, et al. 2022). Severe complications include uterine prolapse and inversion, but this is extraordinarily rare (Yuan, Chen, et al. 2021). Tumor markers are often within normal ranges.
IMAGING
Imaging studies of pelvic tumors help guide diagnosis, management, and if necessary surgical treatment. Ultrasound is the first-line imaging modality of any pelvic mass (Johari, Koshy, et al. 2014). For lipoleiomyomas, ultrasound will show a well-circumscribed, heterogenous hyperechoic mass with hypoechoic ring on or in the uterine wall, with minimal vascularity (Yuan, Chen, et al. 2021). Computed tomography (CT) can better show the location of the lesion, as well as tissue components such as adipose tissue. On CT, the lipoleiomyoma appears as a rim of myometrium surrounding the tumor with intralesional adipose tissue. However, there is a possibility that exact location of the mass may not be evident on CT, as adnexal masses may appear as arising in the uterine wall and vice-versa (Wilke, Benson, et al. 2022; Johari, Koshy, et al. 2014). Magnetic resonance imaging (MRI) is the best modality for describing the architecture and location of the mass. On MRI, the tumor has high intensity on T1- and T2-weighted images, with slightly increased intensity than the surrounding skeletal muscle. Fat suppression techniques can confirm the presence of any fatty component (Manjunatha, Ramaswamy, et al. 2010; Wilke, Benson, et al. 2022). Although radiologic studies can help guide management, histopathological examination is required for definitive diagnosis (Manjunatha, Ramaswamy, et al. 2010; Wilke, Benson, et al. 2022).
HISTOPATHOLOGY
Histopathological examination includes a mixture of bland, spindle-shaped smooth muscle cells without atypia, mature adipocytes, and fibrous tissue (Yuan, Chen, et al. 2021; Manjunatha, Ramaswamy, et al. 2010). The adipocyte component may be as small as 5% or as large as 95%, but a fatty component of greater than 50% is usually observed. Mitotic activity, nuclear pleomorphism, lipoblasts, or atypical cells require further evaluation for malignancy, such as liposarcoma. Myxoid degeneration with or without cystic change, hyaline, and calcification may be seen in benign lipoleiomyomas (Yuan, Chen, et al. 2021). Immunohistochemistry demonstrates adipocytes strongly positive for S100, vimentin, and estrogen/progesterone receptors (ER/PR) with low Ki-67 activity and weakly positive smooth muscle actin (SMA) expression. The smooth muscle cells demonstrate strong positivity for SMA and desmin with partial positivity for ER, PR, and CD34 (Yuan, Chen, et al. 2021). The expression of ER and PR on adipocytes supports the association between hyperestrogenic states and growth, as well as a possible gynecologic origin for the adipocytes (Wilke, Benson, et al. 2022).
DIFFERENTIAL DIAGNOSIS
Differential diagnosis of fatty tumor of uterus includes lipoleiomyoma, mature ovarian teratoma, benign lipoma, degenerated traditional leiomyomas (benign or malignant), or liposarcoma (Manjunatha, Ramaswamy, et al. 2010; Wilke, Benson, et al. 2022). There have been reports of other gynecological malignancies co-existing with lipoleiomyomas, such as liposarcoma arising within a lipoleiomyoma, cervical cancer, or endometrial cancer.
MANAGEMENT
Treatment of lipoleiomyomas is dependent on the patient’s symptoms, if any. If asymptomatic, these patients can be managed with close observation alone. Careful follow-up and repeat imaging is also necessary to evaluate the rapid growth rate of the tumor and the high possibility of liposarcomatous change within the tumor, compared with traditional leiomyomas. For symptomatic patients, hysterectomy is preferred (Wilke, Benson, et al. 2022). Tumor-to-tumor metastasis is well-documented in uterine lipoleiomyomas, where malignancies may be found within the benign tumor. Several cases involving patients with a history of malignancy where breast and gastric adenocarcinoma was found within the uterine lipoleiomyoma have been documented (Kiyokoba, Yagi, et al. 2015). Clinicians and pathologists should be aware of this possibility in patients with a history of malignancy (Yuan, Chen, et al. 2021). If there is a question of malignancy, surgical management is recommended.
CONCLUSION
Lipoleiomyomas are uncommon benign entities, occurring most commonly in post-menopausal women, similarly to uterine fibroids. While asymptomatic patients can be managed conservatively, these tumors can cause vaginal bleeding, pain, and urinary or fecal incontinence and can be definitively treated with hysterectomy. While imaging is necessary to initially characterize the lesion and determine malignancy concern, histopathologic diagnosis remains the gold standard for diagnosis. Lipoleiomyomas are associated with other gynecologic malignancies, metabolic disorders, and rarely tumor-to-tumor metastasis. For this reason, careful clinical evaluation and surgical management are required for complete evaluation of the patient.