
Condensation
This is a case describing a patient with idiopathic splenomegaly who required a combined cesarean section with splenectomy due the risk of imminent splenic rupture.
Brief Description
- This case is reported due to the rarity of idiopathic massive splenomegaly which has led to a paucity of management guidelines and recommendations.
Key Findings
-
Indications for delivery in this patient’s case included constant pain with concern for imminent splenic rupture, hemodynamic instability, and worsening pancytopenia.
-
The patient’s pancytopenia in the setting of idiopathic massive splenomegaly drastically improved following splenectomy.
Teaching Points
-
A combined cesarean with splenectomy proves safe with little impact on short-term maternal and neonatal outcomes (other than those of preterm delivery).
-
Future research is needed to further evaluate etiologies of splenomegaly in pregnancy and to establish clear delivery indications for these patients.
-
Prospective studies are needed to assess long-term impacts on both mother and child following a combined splenectomy and cesarean delivery in the setting of pancytopenia.
Introduction
To date, there is limited knowledge of patients with idiopathic splenomegaly in pregnancy, and the literature lacks cases of a combined cesarean section with splenectomy. The documented cases of splenomegaly in pregnancy often have infectious etiology such as that of malarial infection or an autoimmune component such as idiopathic thrombocytopenic purpura (Singhal et al. 2018). This condition is life-threatening and complicates medical management, but its rarity has led to a paucity of management guidelines for patients with idiopathic splenomegaly in pregnancy.
Methods
This study is a case report with a review of the current literature on the reported cases of splenomegaly in pregnancy, splenectomy in pregnancy, and cesarean section with splenectomy. This case describes a history of pancytopenia and massive splenomegaly in a pregnant patient who underwent extensive workup with no clear etiology. This case additionally describes the course of care for this patient, including a combined cesarean section with splenectomy. We searched PubMed for all English language articles from 2000 to 2023, with search terms including “splenomegaly in pregnancy,” “splenectomy in pregnancy,” and “cesarean section and splenectomy.”
Case
The patient was a 33-year-old gravida 9 para 8104 at 32 weeks 2 days gestation by 17-week ultrasound, with an estimated due date of 12/9/2023. This pregnancy was complicated by pancytopenia, splenomegaly, and a history of fetal demise.
She had a prior hospital admission of seven days for hemoptysis in the setting of pancytopenia (on admission: white blood cells 1,600; hemoglobin 7.0; platelets 24,000) and left-sided abdominal pain. She was found to have splenomegaly, for which our differential diagnoses are listed below in Table 1. An extensive workup for sources of splenomegaly was completed at the time including an inconclusive bone marrow biopsy and a wide range of autoimmune panels which were all negative. During this admission infectious disease was consulted, and they evaluated for any infectious sources. One nutritional deficiency was found at that time- iron deficiency- which was corrected with 900 mg intravenous iron sucrose. As she neared day six and seven of admission, her splenomegaly and pancytopenia remained stable, and her left-sided pain resolved so she was discharged with close outpatient follow-up.
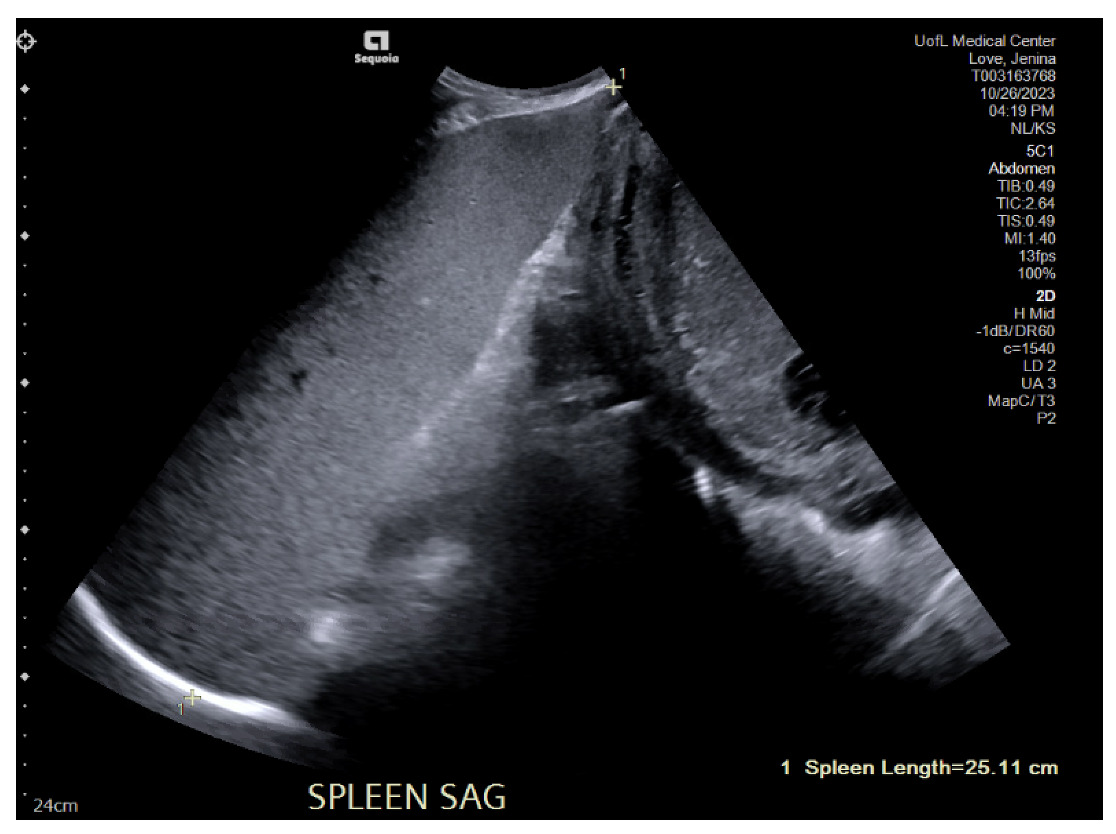
This patient returned to care one month and twenty days later with complaints of constant left-sided abdominal pain. The hematology/oncology, infectious disease, and general surgery teams were consulted. The specific workup performed by Infectious Disease during both admissions can be referenced below in Table 2. The hematology/oncology team was concerned about her massive splenomegaly, now 25 centimeters as demonstrated in Figures 1A and 1B, and the potential for spontaneous rupture. This admission, hematology/oncology completed additional workup with Next Generation Sequencing (NGS) panel, BCR-ABL mutation, JAK exon 12, 13. These returned as negative, and our multidisciplinary team concluded that the cause of splenomegaly could be determined from surgical resection and pathology analysis.

In consultation with surgery, it was recommended to coordinate a combined case for cesarean delivery and splenectomy as there was growing concern for spontaneous rupture of her spleen. Three units of platelets were given starting about three hours before this surgery and continued during surgery. During the operation, a vertical midline incision was made. Once peritoneum was entered, ultrasound was sterilely performed, and the fetus was found to be spine up. Once the uterus was entered, legs were delivered first then followed by the back and head delivered atraumatically. A midline vertical incision with breech delivery was performed to reduce pressure put on the spleen. After delivery of the baby and passage to Neonatal Intensive Care Unit (NICU), the uterus was closed and found to be hemostatic.
On passage of the baby to the NICU, he was noted to have minimal respiratory effort and continuous positive air pressure (CPAP) was started at 1 minute of life. His heart rate was continuously below 100, so positive pressure ventilation (PPV) was started at 1.5 minute of life. His oxygen saturation remained in the fifties, so his oxygen was turned up to 100%. His heart rate improved at 5 minutes of life at which point his PPV stopped, and CPAP was resumed. Baby Boy was weaned to 40% oxygen, at which point he was transported in an incubator while on CPAP. His APGARs were 5,7, and 8 at 1, 5, 10 minutes respectively.
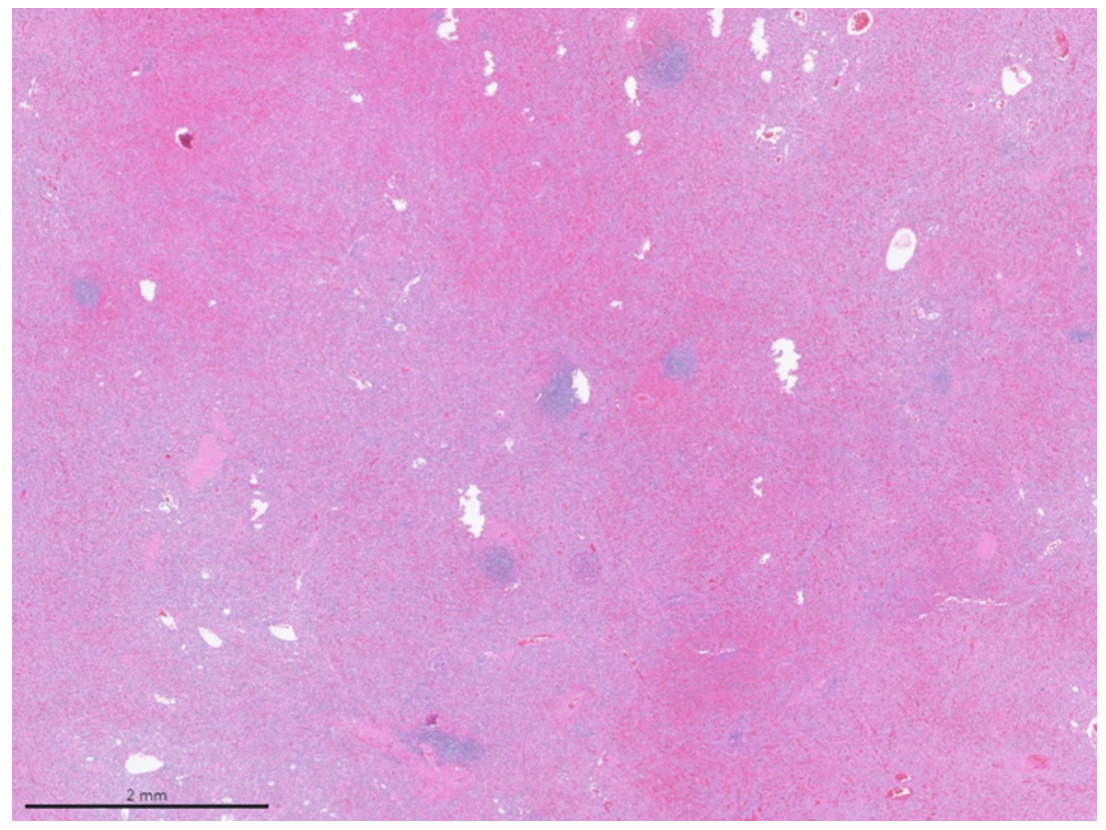
Following cesarean, the splenectomy was begun, in which the midline laparotomy was extended superiorly, then the spleen was medialized and extracted (Figure 2A). A nineteen-french blake drain was placed in the splenic bed and the incision was closed. Her splenic pathology later returned as “hemorrhagic splenic parenchyma with splenic parenchyma with red pulp expansion, foci of fibrin minimal extramedullary hematopoiesis and small hemangioma.” Immunohistochemistry of splenic pathology was positive for CD20 in small B cells, CD3 positive in small T cells, CD30 negative. Epstein-Barr Encoding Region In-Situ Hybridization (EBER-ISH) to evaluate for detection of EBV in the tissue was negative. See Figure 3A below for this pathology and histology.


Baby Boy remained in NICU for recovery, requiring additional oxygen support as well as surfactant due to prematurity. However, he was extubated at day of life 1 and was weaned to room air at one week old. His initial glucose was low at 13, but he had normal glucose values following this. Baby has remained without any neurologic concerns, without signs of sepsis, and continuing to increase in oral feeding tolerance. Baby continues to improve in his status despite placental pathology revealing signs of chronic chorioamnionitis. He was discharged at 34 weeks gestation after 22 days in the NICU with iron and caloric supplements, but otherwise no additional workup or treatments planned.
The patient continued to improve following her combined operation. Her drain output was minimal and was removed without complication. Her pancytopenia greatly improved following her splenectomy. Her pre- and post-surgical blood count values are as follows: white blood cells 2,000 to 9,400; hemoglobin 9.8 to 11.2; and platelets 26,000 to 56,000. Her hemoglobin remained stable, and platelets trended upwards over the next several days. On discharge, her white blood cells were at 7,000, hemoglobin was 8.7, platelets were 477,000. She was able to ambulate, tolerate a regular diet, and she continued to meet other postoperative milestones. Upon discharge, she received the appropriate post-splenectomy vaccines to protect her against encapsulated organisms. To date, she has continued to remain stable in outpatient follow-up.
Discussion
Principal Findings
In this patient’s case, an extensive infectious disease workup was completed in addition to evaluation for hematologic, inflammatory, and neoplastic causes with no clear etiology uncovered. At a gestational age of 34 weeks and 2 days our multidisciplinary team proceeded with cesarean delivery and splenectomy in the early pre-term. The patient’s pancytopenia improved within hours of spleen removal and has remained stable to date in outpatient follow-up. Baby Boy completed a NICU course of 22 days after requiring some surfactant and respiratory support due to prematurity as well as monitoring due to maternal splenomegaly and thrombocytopenia.
Results
As the patient’s hospital course continued, our teams decided that, due to the risk of spontaneous splenic rupture during the labor process and pushing, it was safer for both mother and baby to proceed with cesarean delivery and splenectomy in the early pre-term. Although there is no delivery indication based on platelet count alone as in the case of gestational thrombocytopenia or other diseases, delivery was indicated in this case due to severe constant pain of the patient, worsening pancytopenia, and concern for imminent rupture of her spleen (ACOG PRACTICE BULLETIN Clinical Management Guidelines for Obstetrician-Gynecologists NUMBER 207 2019). Additionally, a scheduled cesarean delivery allowed for a controlled delivery of the infant, as opposed to an emergent cesarean if this patient had decompensated during admission.
Of note, combined cesarean with splenectomy proved to be very efficacious and safe for both mother and baby. The patient’s pancytopenia improved within hours of spleen removal. Her platelets and hemoglobin drastically increased over the next few days following her surgery and have remained stable to date in outpatient follow-up. At her one week follow-up appointment in clinic, the patient’s midline vertical incision remained clean, dry, and intact without concerns for infection or other complications. As far as her baby’s outcomes: Baby Boy remained in NICU for recovery, requiring additional oxygen support as well as surfactant due to prematurity. However, he was extubated at day of life 1 and was weaned to room air at one week old. Baby has remained without any neurologic concerns, without signs of sepsis, and continuing to increase in oral feeding tolerance. Baby continues to improve in his status despite placental pathology revealing signs of chronic chorioamnionitis.
Although there have been documented cases of splenomegaly in pregnancy due to infectious or autoimmune courses, idiopathic splenomegaly is uncommon (Ali and Eldin 2023). Our differential diagnosis for our patient’s splenomegaly included a range of diagnoses including infectious, hematologic, congestive, inflammatory, and neoplastic etiology as demonstrated in Table 12. Infectious workup as described in Table 2 ruled out potential infectious causes within our differential. With autoimmune panels performed and a relatively normal blood smear (although hypoplastic) and bone marrow sample, hematologic/neoplastic sources were ruled out as well, along with inflammatory. The hope then, was that splenic pathology would provide insight into this patient’s etiology of splenomegaly. Splenic pathology of the patient returned as “hemorrhagic splenic parenchyma with red pulp expansion, foci of fibrin deposition, minimal extramedullary hematopoiesis and small hemangioma.”
Clinical Implications
This case provides novel insight into management of idiopathic splenomegaly in pregnancy and specifically the management of massive splenomegaly (> 8 cm). To our knowledge, there is only one other documented case of combined cesarean delivery with splenectomy (Pol et al. 2017). However, that cesarean was indicated due to failed induction of labor, and the opportunity was taken to perform a splenectomy at the same time due to progressive portal hypertension. Thus, our case provides the opportunity to document an appropriate management and follow-up of a patient post-cesarean and splenectomy. Additionally, this case provides insight into management of pregnant patients when imminent splenic rupture is a concern.
Research Implications
A review of splenectomies performed showed that about 64% of splenectomies performed for splenomegaly provided a definitive diagnosis. About half of these patients had an underlying malignancy, while 1-4% of these patients remained with unknown etiology (Palumbo et al. 2021). Thus, this patient’s case is a rare one, and future research pursuits should be made to determine causes of splenomegaly in pregnancy, any modifiable risk factors for this condition, as well as any alternative treatment options. Further follow-up is also necessary to determine any long-term impacts on patients who undergo this treatment.
Disclosures
The authors report no conflicts of interest.
Corresponding Author:
Samantha L Stone
500 S Preston St
Building A, Suite 210
Louisville, KY 40202
859-583-4047, samanthastone.1@outlook.com