Case Introduction
Anti-N-Methyl-D-aspartate receptor (anti-NMDAR) encephalitis is a condition that presents with signs of altered mental status often quite spontaneously in patients. It can be traced to autoimmune conditions or certain tumors that produce antibodies against the anti-N-Methyl-D-aspartate receptors in the brain. NMDA receptors are expressed on pyramidal neurons all throughout the cerebral cortex as well as in the hippocampus thus influencing the creation of memories. Therefore, the presence of anti-NMDAR encephalitis can cause multiple neurological sequelae that subsequently presents with altered mental status that may progress to seizures and death. Females are more likely to be affected by this disease, especially those in the 25 to 35 year age group. In 2005, four women with age ranges 14-28 were found to have ovarian teratomas as well as memory loss combined with psychiatric changes that eventually was diagnosed as anti-NMDAR encephalitis. This link between teratomas and encephalitis shows a paraneoplastic pattern that has mostly been associated with mature ovarian teratomas in females, although it can happen in males as well. If caught in time, immediate surgical removal of the tumor as well as immunotherapy and steroid treatment can reverse much of the neurological impairment in patients. This is a case report of a patient with a rare immature teratoma and gliomatosis peritonei that will highlight the importance of pelvic imaging early on in the work-up for self-reported abnormal neurological deficits.
Case Description
We present a case of an 18-year-old female with no past medical history that presents to the emergency department (ED) with a gradual bilateral frontal headache associated with double vision, blurry vision, left arm tingling, and claims of her eyes crossing on and off. She also says she had some involuntary movements of her right arm a few days ago. The patient denied frequent headaches but they usually have migrainous features not similar to the current one. On physical examination, her blood pressure was elevated at 149/94 mmHg but all other values were normal including an afebrile temperature of 37.2℃. Her neurological exam showed that she was alert and oriented to person, place, and time and had no focal deficits. Neurology was consulted and computed tomography (CT) without contrast showed normal findings; however, CT with contrast showed abnormal vessels in the left frontotemporal region indicating a possible arteriovenous malformation which was confirmed with a magnetic resonance imaging (MRI) of the head. She was then admitted for further evaluation and started on Keppra for seizure prophylaxis. During her hospital stay, the patient reported tremors of the right hand and had intermittent episodes of diplopia. A cerebral angiogram was then performed two days later which showed an incidental finding of a developmental venous anomaly on the left side. The patient was then discharged three days after her admittance.
Approximately eleven months later, the patient came back to the ED for a reported seizure earlier in the day where generalized shaking occurred and lasted for 15 seconds. She also had postictal confusion. Repeat CT of brain and electroencephalogram (EEG) were normal and it was thought that the venous anomaly was causing a focal seizure so the patient was again started on Keppra and discharged a day later.
The next day the patient came back with her mother, who provided most of the information during her stay, and was admitted for altered mental status and confusion. She had been having some trouble with her memory and concentration along with having no memory of her hospital stay the day before. Her neurological examination at the time was normal. MRI, CT, and EEG of the brain was normal. The next day upon examination, the patient claims she has been hearing music that is not there, having nightmares, and appears very tearful. She was then switched to Ativan and started on Lexapro for concerns of a mood disorder. Over the next few days, she had garbled speech and an aphasic episode. She was not able to sleep for several days and was anxious with tangential speech . On mental status examination, the patient showed some psychomotor agitation, pressured speech, disorganized thought process, and poor insight. She stated “they are coming for me” when asked further questions.
Five days after admission, psychiatry was paged and suggested an evaluation for possible autoimmune/limbic encephalitis thus she was started on intravenous (IV) methylprednisolone and a lumbar puncture was performed. Cerebrospinal fluid (CSF) analysis showed 5 red blood cells/mcL and 92% lymphocytes with a normal value of neutrophils at 6%. A Meningitis/Encephalitis polymerase chain reaction (PCR) panel was negative but IV Acyclovir was started as precaution and Infectious Disease was consulted for a new onset fever and leukocytosis. IV Acyclovir was then discontinued once the herpes simplex virus (HSV) PCR came back negative.
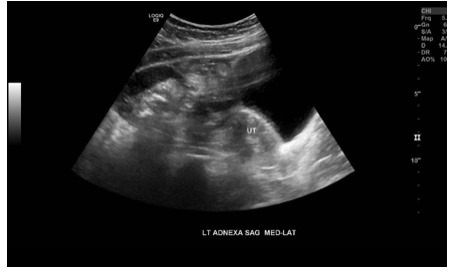
Seven days after admission, the patient was still presenting with severe agitation and attempted to escape the hospital. At this time she discussed having severe pelvic cramps during her menstrual cycles. A pelvic ultrasound was then performed that showed a complex left adnexal structure measuring 13.4 x 12.9 x 8.4 centimeters with areas of echogenicity and posterior acoustic shadowing suggesting a teratoma (Figure 1). The left ovary was also unable to be visualized but the uterus and right ovary were within normal limits. The patient was then investigated for possible anti-NMDA encephalitis and empiric immune globulin 10% (IVIG) was started. Obstetrics and Gynecology was consulted and discussed the ovarian teratoma finding and the paraneoplastic process that can cause anti-NMDAR encephalitis. The anti-NMDAR antibody screening was found to be negative but there was still a high suspicion for this phenomenon and thus surgery was planned.
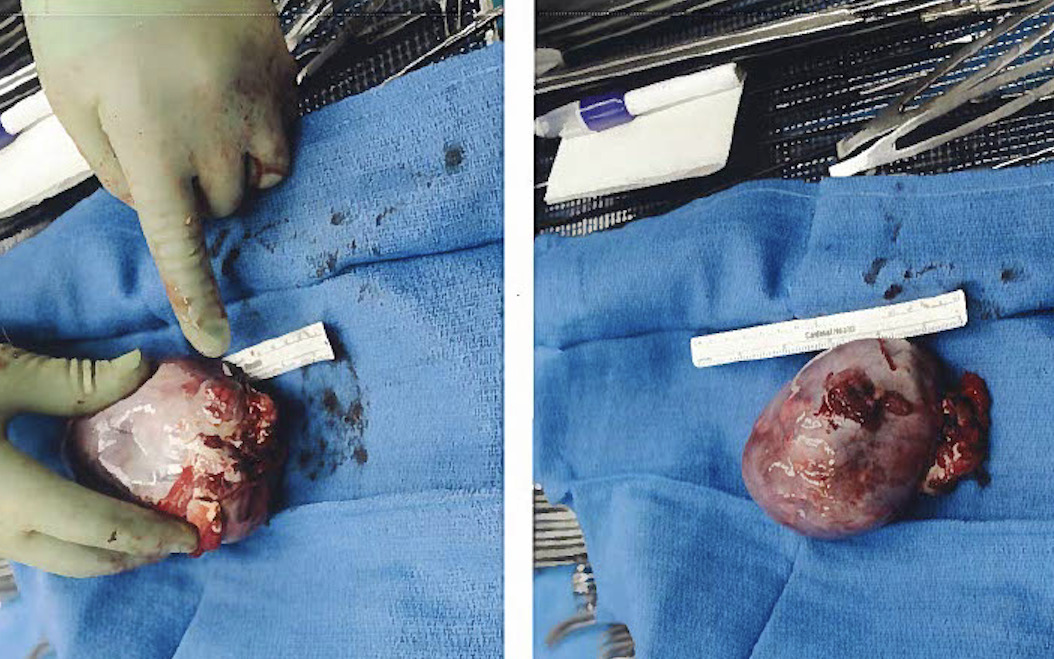
Ten days after admission, a diagnostic laparoscopy with mini laparotomy and left salpingo-oophorectomy was performed on the patient. Cellular glial tissue was present consistent with gliomatosis peritonei. A left high grade immature teratoma was identified at a size of 11.0 x 8.5 x 7.5 centimeters (Figure 2). The glial tissue also showed positive staining for S-100, Neuron-specific Enolase (NSE), and Glial Fibrillary Acidic Protein (GFAP).
Two days status-post surgery, the patient was lethargic but able to answer some questions and vocalize her orientation. An EEG was done at this time and was notable for mild diffuse slowing, a nonspecific finding seen in cases of delirium, sedatives, metabolic encephalopathies, etc.
Three days status-post surgery, the patient was found screaming in the hallway and she claimed to be hearing music again. At this point, she had finished seven days of IV steroids and five days of IVIG. She also had an episode of atrial fibrillation with RVR, which cardiology concluded was likely due to delirium. The patient underwent a CT chest with contrast which demonstrated bilateral effusions but no evidence of malignancy was found.


Case Discussion
Since its discovery, there have been over 500 cases of Anti-NMDAR encephalitis observed in literature. Anti-NMDAR encephalitis is the most common type of encephalitis compared to each individual viral encephalitis. In a systematic review of 119 articles regarding cases of Anti-NMDAR encephalitis, it was found that 74% of cases were traced back to a mature ovarian teratoma. Thus, this form of encephalitis with rapid psychiatric and neurologic changes, affects women disproportionately, especially those between the ages of 12 and 45 with a median age of 21. Previous cases of anti-NMDAR encephalitis were said to have a viral-like prodrome with headache, fever, vomiting, nausea, and fatigue. Our patient was 18 when she was presented with her first headache and vision abnormality however, she lacked other common infectious signs. Additionally, more of the acute psychiatric features are said to commonly present shortly after the initial prodrome in less than three months time. On the contrary, this case showed the patient presenting almost a year later with a neuropsychiatric phase that began with seizures. The presence of seizures is frequent with one study showing 76% of patients with anti-NMDAR encephalitis having generalized tonic-clonic seizures followed by either focal seizures, status epilepticus, or epilepsia partialus continua. The later symptoms of memory loss, confusion, paranoia, and auditory hallucinations seen in our patient are also typical of others with anti-NMDAR encephalitis and associated teratoma.
Less than 1% of ovarian cancers are immature teratomas. They usually occur in women under the age of 20 and are likely to be malignant in affected individuals. It is a rare tumor made up of the three germ layers: ectoderm, mesoderm, and endoderm. The most common tissue present is neural and thus can possess elements that tie back to the central nervous system. Mature teratomas, however, are the predominant subtype to be associated with anti-NMDAR encephalitis with one review showing 74% of cases that had histological typing showing a mature pattern. In addition, patients with mature teratomas tended to have a longer time length from presentation to surgery with a mean of 71.4 days versus those with immature teratomas (mean of 39.4 days from presentation to surgery). In our case, the patient fell into the typical age group of immature teratoma incidence and had a significantly shorter duration of 10 days from presenting with altered mental status to surgery.
Another unique aspect of this case was the lack of detection of Anti–NMDAR antibodies. In one study of 489 patients with Anti-NMDAR encephalitis, 15% were found to have undetectable antibodies. This negative group had an older mean age of onset of 23.5 years versus the positive group with a mean of 20.5 years. One hypothesis for this negative finding was that the antibody titer was too low for detection and thus produced a milder form of encephalitis. For example, in the same study, only 60% of the negative group were likely to develop seizures versus 73% in the seropositive group. It would be interesting to assess if titers may have been detectable at some point during the course of our patient’s workup or if testing again with a different technique such as a commercial cell-based assay would provide different results.
Our patient’s findings of lymphocytic pleocytosis in the CSF is consistent with other reports of anti-NMDA encephalitis. This elevated level of leukocytes in the cerebrospinal fluid is an indicator of some form of inflammation occurring. Thus, an early CSF analysis in a patient with signs of encephalitis could lead to a quicker diagnosis.
In conclusion, ovarian teratoma should be investigated in younger females coming in with signs of altered mental status. Many females come in with neuropsychiatric symptoms and may be diagnosed with a mood disorder when admitted. However, the similar symptoms between anti-NMDAR encephalitis and psychiatric conditions shows the importance of early tumor detection and removal. A pelvic ultrasound should be performed immediately for young females with signs of altered mental status even before an anti-NMDAR antibody screening is performed. This simple imaging could help with early diagnosis and surgery with quick recovery for those with this unique form of encephalitis.