

Background
Hemothorax is the accumulation of blood in the pleural space. The majority of this rare and life-threatening phenomenon are due to blunt or penetrating trauma to the thorax or abdomen, but other causes include iatrogenic, vascular, coagulopathies, infectious and neoplasia (Pumarejo Gomez and Tran 2023). Severity is classified by blood volume collection; minimal is less than 400 milliliter (mL), medium is 400-1000 mL, and massive is greater than 1000 mL (Boersma, Stigt, and Smit 2010). These patients classically present with respiratory distress and tachypnea, and the differential diagnosis includes pulmonary embolism, pneumothorax, and cardiovascular, esophageal and musculoskeletal injuries. The work up is as varied and includes laboratory data, electrocardiogram, and radiographic images such as chest X-ray, ultrasound and/or CT. Treatment options consist of thoracostomy, thoracentesis (bedside or by Interventional Radiology), video-assisted thoracic surgery, thoracotomy or expectant management as guided by the patient’s hemodynamic stability and symptoms (Zeiler et al. 2020). Prognosis is related to severity and if there are any complications from the hemothorax itself or treatments.
An extensive literature review was productive of a few cases of spontaneous hemothoraces in pregnant and postpartum patients. The etiologies in these cases have ranged from ruptured pulmonary arteriovenous malformations to fenestrations in the diaphragm leading to surgical blood loss from the abdomen flowing into the thorax (Zamaniyan et al. 2022; Vaughan, Hooper, and Duffy 2005). In non-pregnant patients, endometriosis lesions have also been implicated. The case presented in this paper is the only reported case of a spontaneous hemothorax in the immediate postpartum period without evidence of typical causes as noted above.
Case Report
The patient is a 42-year-old gravida 16 para 2-2-12-4 woman status-post scheduled repeat low transverse cesarean section at term. Her past medical history was significant for recurrent pregnancy loss with a history of intrauterine fetal demise at 16 weeks and 20 weeks gestation. She had had a normal antiphospholipid antibody syndrome work-up. She took Synthroid 75 mcg for hypothyroidism with a recent thyroid stimulating hormone level of 0.599. She also had a history of asthma for which she had not used an inhaler in one year. She also took magnesium oxide for migraine headaches and had a remote history of latent tuberculosis for which she was treated in 2001. Her surgical history was notable for three prior uncomplicated cesarean sections for breech presentation and non-reassuring fetal heart tracing. She also had had a tonsillectomy, wisdom teeth removal, peroneal tendon repair, and laparoscopic lysis of adhesions and fulguration for endometriosis. She had used Lupron prior to pregnancy for many years due to her endometriosis.
Her pre-operative hemoglobin and hematocrit were 10.9 and 33.4. She received gentamicin and clindamycin intraoperatively for antibiotic prophylaxis given an anaphylactic allergy to penicillin. Her scheduled repeat cesarean section was notable for significantly dense scar tissue around the rectus muscles and a difficult to identify lower uterine segment. Her prior bladder flap had not been reapproximated and had healed such that the bladder was adhered to the right lower uterine segment. Uterine reactive changes were seen and attributed to endometriosis. Her lower uterine segment was also extremely thin, and the patient was strongly advised to never attempt a vaginal delivery in the future. Her surgery was otherwise uncomplicated with a quantitative blood loss of 536 mL.
Post-operatively the patient had persistently low blood pressures (primarily 80s/60s) and an episode of painful emesis (approximately 1000 mL). She otherwise remained normocardic and was saturating well on room air. She was given 1 liter of lactated ringers (LR) fluid and Reglan 10 mg IV, however approximately one hour later, her blood pressure remained low (83/66) and she began to look pale with pre-syncope. She remained normocardic with a heart rate at 86 and SpO2 at 98%. She was afebrile throughout her entire clinical course.
Upon evaluation, the pt appeared very pale and stated that she was tired. She could not lift her extremities and reported blurry vision. She denied chest and abdominal pain, shortness of breath, or any repeated nausea or vomiting. A bedside FAST exam was performed and negative. She was appropriately tender on exam of the abdomen with no guarding or rebound. She was given 1 unit Packed Red Blood Cell (PRBCs) due to concern for acute hemorrhage along with 2 L of fluid. Preop Complete Blood Count (CBC) was 10.9/33.4 and had dropped to 9/27.9 before administration of PRBCs. After receiving the fluids and 1U PRBCs the pt appeared significantly less pale and more alert, stating that she “felt much better.” She continued to feel better throughout the morning and her blood pressure remained stable at 90-100s/50-60s.
Repeat CBC approximately 4 hours after transfusion showed H/H of 8.8/26.7. Over the course of the day, she started to report some right chest tightness and pain that radiated to her neck, shoulder, and rib. EKG was normal and the patient was given 500mL Lactated Ringer bolus. That evening she reported worsening of her chest pain and new onset SOB with diaphoresis noted on exam. Vitals stable with BPs 90s/50s, patient was normocardic with normal pulmonary findings. Repeat EKG was normal. CBC repeated and imaging ordered given concern for possible PE.
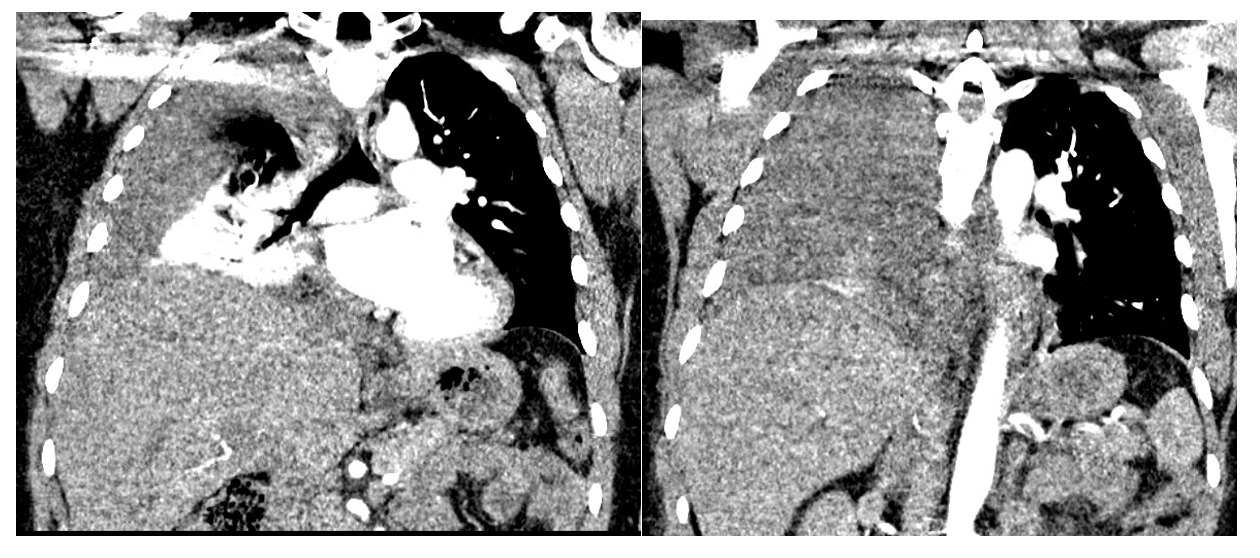
Chest CT showed large right pleural effusion consistent with a hemothorax and possible pulmonary embolism of distal vessels which was thought to be secondary to artifact after discussion with radiology. (Figure 1 and 2). Abdominal/pelvic CT showed significant heterogeneous intrauterine material and findings consistent with post-op c-section.
The patient had a steadily declining Hemoglobin/Hematocrit (H/H) of 10.9/33.4 preoperatively to 6.9/20.7 on evening of postoperative day 2. She was given a 2nd unit PRBC with improvement of her H/H to 8/23. Pt clinically had very minimal vaginal bleeding since surgery and her uterus was noted to be firm at the umbilicus. There was some concern for slow uterine hemorrhage, but the patient was deemed a poor candidate for anesthesia given large pleural effusion in the case of operating room take back. General surgery was consulted who recommended thoracentesis later that day by Interventional Radiology which was performed without issue and notable for drainage of 675 mL of dark bloody fluid. Post-thoracentesis the pt noted some improvement of her shortness of breath but still reported significant chest pain and shortness of breath. We reordered a CT to re-evaluate for clot which was negative however repeat CT showed a significant improvement in fluid present in her right lung (Figure 3).

By postoperative day three she was overall improved, but still noted some shortness of breath and mild pain in the right shoulder. Her lung fields were clear and serial CXR from this time until discharge would show no reaccumulation of fluid. After drainage of pleural effusion, she was noted to have a hemoglobin drop from 8.7 to 7.2 on AM of postoperative day 3. We provided 2 units PRBCs, with H/H now 10.2/29.7<184. and remained stable at that level until discharge. Patient had no further episodes of hemothorax during her recovery and the remainder of her postpartum course was uneventful.
Discussion
Etiologies for her spontaneous hemothorax are ultimately uncertain. This patient’s case is unique in that this hemothorax developed in an otherwise uncomplicated patient without a clear trigger as seen in other cases (Pumarejo Gomez and Tran 2023; Boersma, Stigt, and Smit 2010; Zeiler et al. 2020; Zamaniyan et al. 2022). This case underwent a multi-disciplinary review. Our primary hypothesis was that the patient may have had a small undiagnosed fenestrations that allowed intraoperative blood loss to cause a hemothorax when these spaces were dependent during a cesarean section. This explanation, while possible, would not account for the steadily declining hemoglobin post-operatively. The operating and night team speculated that a vessel may have ruptured and filled the space with blood after her violent episode of emesis. Another possible etiology is a rupture of an endometrial implant which has been previously seen in the literature but there is no good explanation as to why this would have happened during a delivery. Finally a rare rupture of an arterio-venous malformation is possible, and cannot be fully ruled out. Ultimately no one etiology can be confirmed in this case, and this highlights the need for provider to maintain a high index of suspicion for this rare complication even in routine cases where a clear trigger does not always present itself.
Authors Contributions
Eric Michael Schmitt: Primary Author. Chiefly responsible for concept and design of manuscript.
Casey Gentile: Co-Author. Assisted in both manuscript development and in the development of the below presentation
Britteny Randall: Co-Author. Assisted in both manuscript development and in the development of the below presentation
Disclosures
The Author(s) reports no conflicts of interest, and no funding has been received for this work.
This case report has been presented at ACOG Armed Forces District Conference 2024; 2024 October 5-9; McLean, VA.
The views expressed herein are those of the presenter and do not reflect the official policy of the Department of the Army, Department of Defense, Defense Health Agency, or U.S. Government.
Disclaimer
Eric M SCHMITT, MD; Britteny RANDALL, MD; Casey GENTILE, MD; are employed by the Armed Forces.