
Background
Ectopic pregnancy, defined as any pregnancy occurring outside of the uterine cavity, accounts for approximately two percent of pregnancies (“Ectopic Pregnancy—United States, 1990-1992” 1995). While ectopic pregnancies are well described in the literature, they are still a significant cause of morbidity and mortality, and in 2012-2013, ruptured ectopic pregnancies accounted for 2.7% of all pregnancy related deaths (Creanga et al. 2017). Therefore the study of ectopic pregnancies, and especially studying atypical presentations of this finding in the setting of expanded IVF use, is still an important area of research that has been growing.
The most common site of an ectopic pregnancy is the fallopian tube, with over 90% of cases being found in this anatomical region (Bouyer et al. 2002). Many female patients presenting to the emergency department with abdominal pain and a new pregnancy finding have an ultrasound focusing on intrauterine and tubal/ovarian findings in an effort to either diagnose a new pregnancy or an ectopic in the most expected initial location. However, this evaluation does not take into account rare alternative locations where ectopic pregnancies can be found. We describe a rare case of an abdominal ectopic pregnancy implanted on a pedunculated subserosal uterine fibroid.
Abdominal pregnancies are a rare form of ectopic pregnancies accounting for only 1%-4% of all ectopic pregnancies (Ekele et al. 2005). On review of the current literature, there has been only one existing case report of an abdominal ectopic pregnancy implanted on a pedunculated subserosal uterine fibroid (Sato et al. 2019). Our case is unique in that the previous case report describes an IVF assisted pregnancy, which is a known risk factor for ectopic pregnancies. Our patient had a spontaneous pregnancy with no ectopic risk factors and no prior uterine surgeries but still had an ectopic in this rare location.
Manuscript
A 30-year-old female, gravida 2, para 1 (vaginal birth), with no significant medical history presented to the emergency department at approximately 4 weeks gestation after sudden onset of sharp stabbing midline and left lower quadrant abdominal pain. Patient denied any vaginal bleeding.
On exam, her vital signs were within normal limits. Abdominal exam revealed significant tenderness to palpation throughout the lower abdomen along with rebound tenderness. Laboratory evaluation revealed a hemoglobin of 11.9 g/dL and β human chorionic gonadotropin of 1,686 mIU/mL. Transabdominal and transvaginal ultrasound revealed a normal appearing uterus measuring 9.6 x 5.0 x 5.5 cm with no identified intrauterine gestational sac or yolk sac. There was noted to be a non-specific heterogenous, nonvascular mass of the right adnexa with no pelvic free fluid noted (Figure 1).

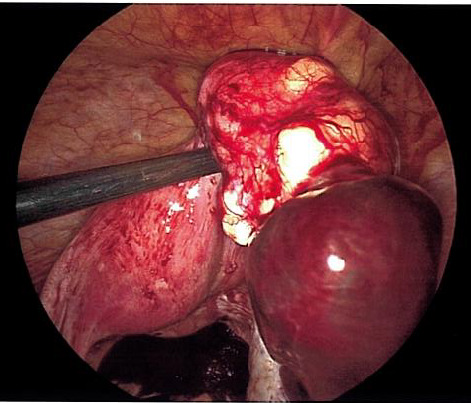
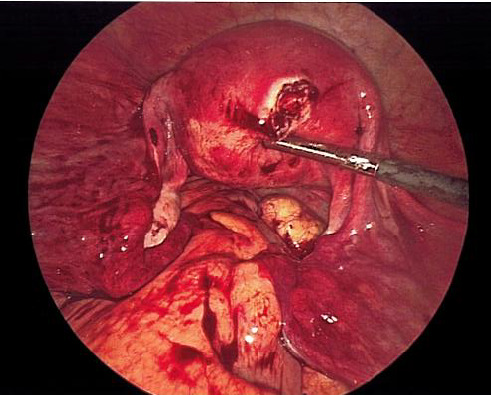
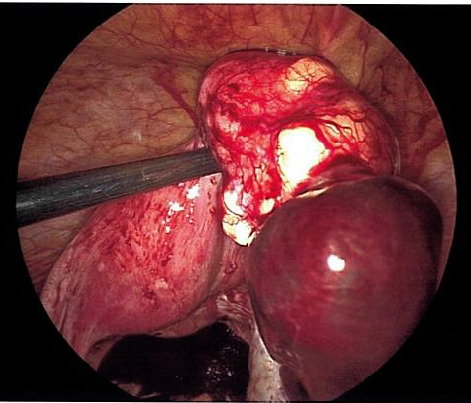
The patient was taken urgently to the operating room for diagnostic laparoscopy due to concern for right adnexal ectopic pregnancy. Upon entry into the abdomen, hemoperitoneum was noted extending into bilateral paracolic gutters. Following removal of this clot, a ruptured ectopic pregnancy was identified at the inferior pole of a 4 cm pedunculated fibroid arising from the posterior fundal surface of the uterus with active bleeding (Figure 2). This ectopic pregnancy revealed no involvement of bilateral adnexa. Pelvic survey revealed normal bilateral fallopian tubes and ovaries. The pedunculated fibroid and ectopic pregnancy were resected with the Ligasure impact device and removed from the abdomen by two separate Endocatch bags. The base of the myomectomy (Figure 3) was oversewn with 2-0 vicryl for additional hemostasis.

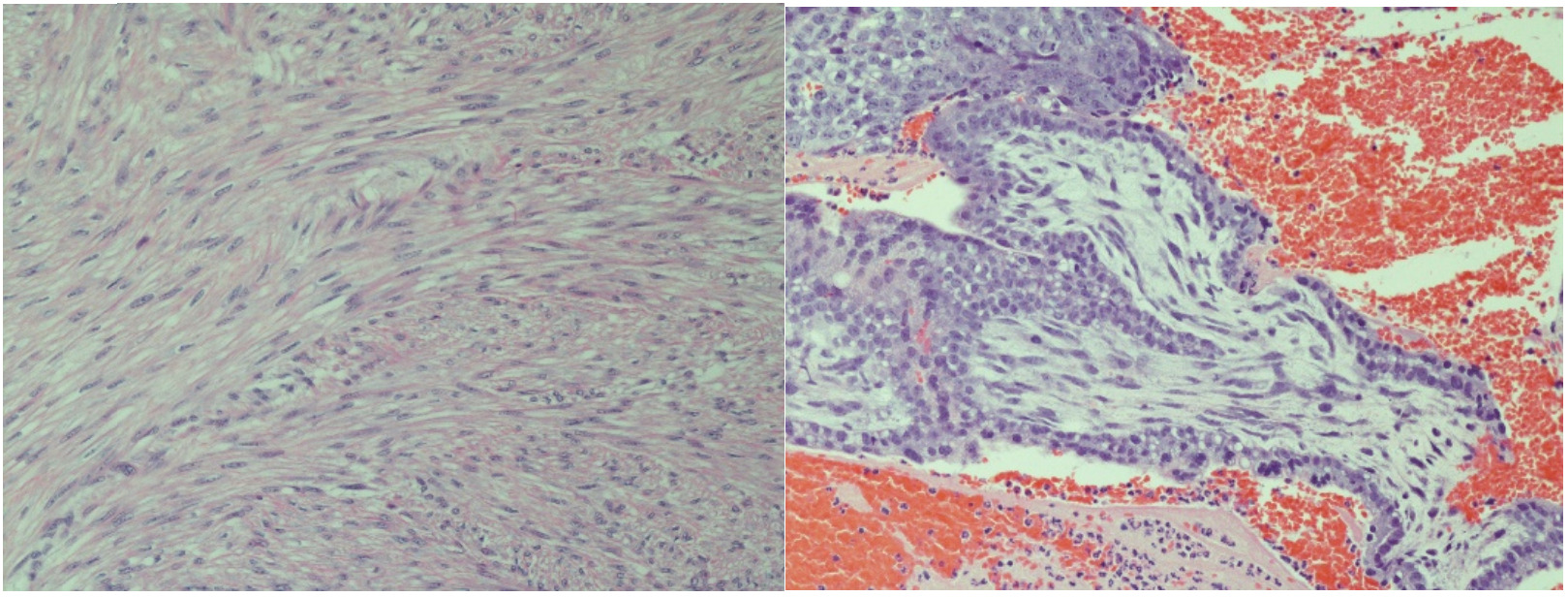
The patient had an uncomplicated postoperative course and was meeting all expected postoperative milestones at her 6 week follow-up. Surgical pathology confirmed diagnosis with visualized rare immature chorionic villi and syncytiotrophblasts, consistent with products of conception and leiomyoma. Her β human chorionic gonadotropin was followed to a negative value (2.7 mIU/mL) which occurred at 2 weeks postoperatively.
Discussion
We describe the first case of an abdominal ectopic pregnancy implanted on a pedunculated subserosal uterine fibroid in a natural pregnancy. This case has important implications for future gynecological care.
Our case serves as an important example of an abdominal ectopic that is not associated with IVF or other ectopic risk factors. Existing literature, such as a systemic review from Yoder et al describe 29 abdominal ectopic pregnancies that were strongly associated with tubal infertility treated by IVF, or prior tubal surgery (Yoder et al. 2016). While these are known risk factors for ectopic pregnancy in general, these also seem to be risk factors for atypical presentations of ectopic pregnancies specifically. However, providers should not ignore the possibility of these atypical presentations even in medically straightforward patients. Our patient presented without a history of uterine surgeries, IVF use, or any risk factors for ectopic pregnancy. Despite this, we found only the second reported ectopic pregnancy in a pedunculated subserosal uterine fibroid which required a unique surgical approach to safely remove. Ultimately, gynecological surgeons must have a high index of suspicion for these atypical presentations and be ready to adjust to the surgical findings as they present.
._bundles_of_smooth_muscle_consist.png)
Authors Contributions
Caitlin Sledge: Primary Author. Chiefly responsible for concept and design of manuscript.
Amanda Tashjian: Co-Author. Assisted in both manuscript development and in the development of the below presentation
Karen Strenge: Co-Author. Assisted in both manuscript development and in the development of the below presentation
Eric Michael Schmitt: Editor: Prepared final manuscript for publication
Disclosures
The Author(s) reports no conflicts of interest, and no funding has been received for this work.
This case report has been presented at ACOG Armed Forces District Conference 2025. ACOG Armed Forces District Conference 2025; 13SEP-17SEP 2025; Norfolk, VA.
The views expressed herein are those of the presenter and do not reflect the official policy of the Department of the Army, Department of Defense, Defense Health Agency, or U.S. Government.
Disclaimer
Caitlin SLEDGE, MD; Amanda TASHJIAN, MD; Karen S STRENGE, MD; Eric M SCHMITT, MD; are employed by the United States Armed Forces.