
INTRODUCTION
The incidence of rectal foreign bodies is increasing in the United States (Loria et al. 2023). Of patients who present with retained rectal foreign bodies, most are male (Coskun et al. 2013). Objects can be retained in the rectum after oral ingestion or, more commonly, are inserted transanally (Coskun et al. 2013).
Rectal foreign bodies pose risks including impaction, peritonitis, and perforation. Methods of removal include extraction manually, endoscopically, or via laparotomy (Coskun et al. 2013; Johnson and Hartranft 1996). Many patients will ultimately require colostomy with surgical interventions (Cohen and Sackier 1996).
The literature documents the use of obstetric instruments being used to remove rectal foreign bodies including vacuum delivery systems and, more rarely, obstetric forceps (Johnson and Hartranft 1996; Sajjad and Paish 2023; Hussain Andrab et al. 2009; Sparks et al. 2015). This case will review the transanal extraction of a rectal foreign body using Tucker-McClane obstetric forceps.
CASE REPORT
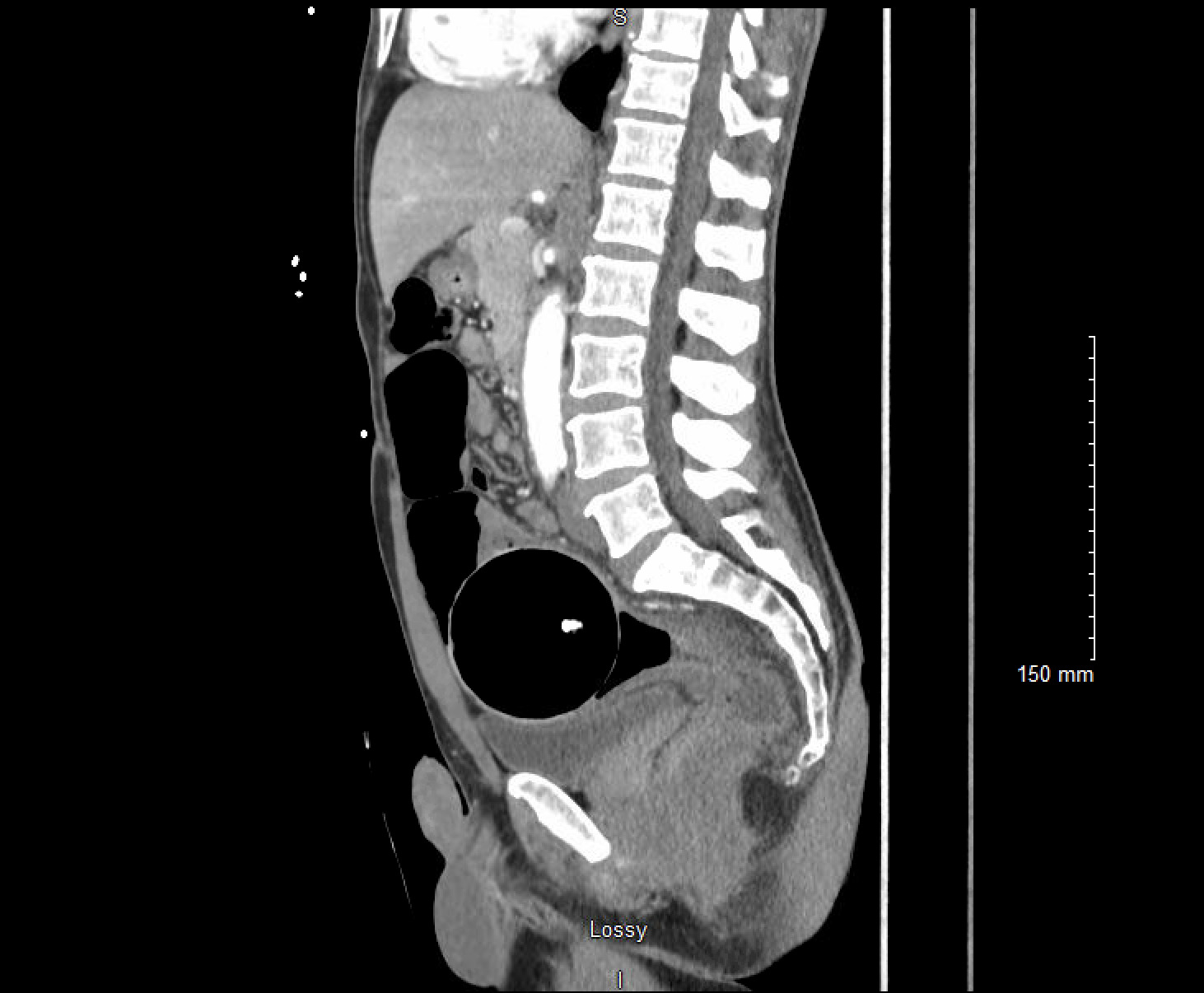
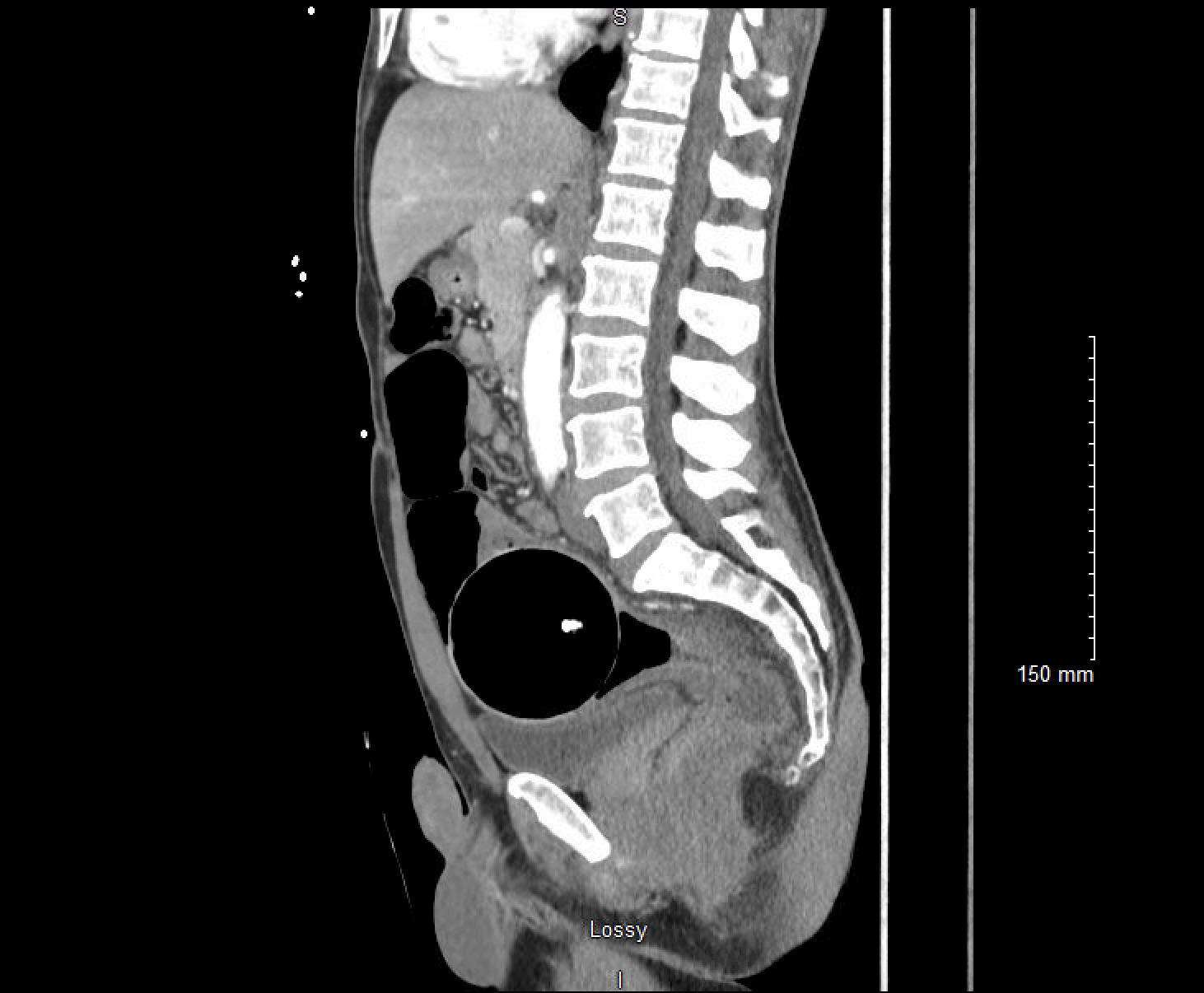
An adult male presented to the Emergency Department with a retained rectal object. On presentation, the patient was clinically stable, though he reported feeling constipated and bloated after four days with the object in situ. A CT abdomen and pelvis with intravenous contrast was performed which demonstrated a 8.2 cm spherical foreign body in the distal sigmoid colon with thickening of the distal sigmoid colon and rectum. There was no evidence to suggest perforation. (Figures 1-2) The retained object was a sphere made of hard plastic with a light inside. A chain attached to the sphere had broken off–not allowing the patient to remove the object himself. Initial attempts made to evacuate the object in the emergency department included the use of an obstetric vacuum delivery system; however, the patient was unable to tolerate these attempts. He was then taken to the operating room for removal under general anesthesia. In the dorsal lithotomy position, the sphere was able to be palpated. Given the hard material of the object, it was not able to be grasped or penetrated with Kocher clamps or myoma screws. An obstetrical vacuum was able to guide the object caudally into the rectum, but the vacuum was not able to fully extract the object. Ultimately, an obstetrician-gynecologist applied Tucker McClane obstetric forceps around the object and was able to successfully deliver the sphere. A general surgeon subsequently performed endoscopy to confirm there were no rectal or sphincter lacerations. The patient was able to be discharged home the same day.

DISCUSSION
In the management of rectal foreign bodies, lesser invasive techniques should be utilized before more invasive alternatives (Sajjad and Paish 2023). Imaging via either abdominal X-ray or contrast enhanced CT of the abdomen should be performed if the patient is hemodynamically stable in order to assess size, position, location, and for possible perforation (Tarasconi et al. 2021). Often rectal foreign bodies are unable to be manually extracted either due to position, shape of the object, or due to patient intolerance. These patients should be taken to the operating room for removal under anesthesia (Tarasconi et al. 2021).
As the incidence of rectal foreign objects continues to rise, the need for wider methods of extraction will be helpful in avoiding more morbid procedures such as laparotomy and colostomy for removal. In cases where a rectal foreign body is hard, smooth, and spherical, traditional methods of removal either manually or endoscopically can be especially difficult due to lack of purchase with traditional instruments.
On review of the literature surrounding using obstetric instruments for removal of rectal foreign bodies, vacuum delivery devices are more commonly used compared to obstetric forceps (Coskun et al. 2013; Johnson and Hartranft 1996; Sajjad and Paish 2023). There are some case reports of extraction with obstetric forceps using both a single blade technique as well as traditional method with two articulated blades (Hussain Andrab et al. 2009; Sparks et al. 2015).
Similar to use of obstetric forceps in a vaginal delivery, there is a risk of laceration to the gastrointestinal tract; therefore, the use of endoscopy after extraction should be used to assess for these potential complications (Tarasconi et al. 2021). The patient in our case had no lacerations or evidence of perforation. They were able to avoid more invasive surgery and were discharged home the same day.
Emergency medicine physicians and general surgeons are most commonly the providers who perform extractions of rectal foreign bodies; however, there may be a role for obstetrician-gynecologists. In our case, the retained object was difficult to remove due to its size, shape, and material. A board certified obstetrician-gynecologist, who is trained in the insertion and articulation of obstetrical forcep blades, successfully removed the rectal foreign body without additional damage to the rectum or anus. Obstetric forceps should be considered as a potential instrument for extracting retained rectal foreign bodies in certain situations.