1. Introduction
1.1. Study Rationale
Although the number of voluntary pregnancy terminations has decreased since the initial federal legalization in 1973,1 abortion care is still a common and essential form of healthcare sought by many patients, ranging from ages 15-44.2 In Michigan specifically, the decrease in abortion cases has been coupled with a shift from a physician’s office to a freestanding clinics, with the proportion of voluntary abortions at independent clinics increasing nearly 20% from 2013 to 2014 alone.1 In the State of Michigan, patients could choose between two options for first trimester voluntary terminations of pregnancy: surgical (suction curettage via vacuum aspiration) or medical (induced by mifepristone and misoprostol). With surgical abortions, pregnancy tissue was passed on the day of the appointment in the procedure room; with medical abortions, pregnancy tissue was passed within three days in the privacy of the patient’s own space.
Given the surge in demand for remote care and telehealth visits as a result of COVID-19, the authors hypothesized that there would be an increase in medical abortions over surgical abortions for first trimester voluntary terminations during the pandemic, as seen in abortion pandemic research.3 The State of Michigan enacted a “stay-at-home” executive order on March 24, 2020.4 Although this order allowed exceptions for seeking “tasks that are necessary to health and safety,” it also ordered that “all individuals who leave their home or place of residence must adhere to social distancing measures … including remaining at least six feet from people.”4 The Centers for Disease Control and Prevention reported an estimated 41% of adults avoided urgent or routine medical care during the pandemic.5 If this order were to impact abortion method choice, then it should be anticipated that the number of medical abortions compared to surgical abortions should increase in the months following March 24, 2020. To further correlate medication abortion trends to the pandemic, there should be a stable trend prior to March 24, 2020, and an eventual return-to-baseline after the executive order expired on June 1, 2020.4
1.2. Background
Of the nine independent abortion clinics in Southeastern Michigan contacted for study involvement, only Scotsdale Women’s Center (SWC) agreed to take part in the study. The two types of first-trimester abortion options performed at SWC were surgical abortion using suction curettage and medical abortion using mifepristone and misoprostol. Prior to either procedure, the patient requirements included: ultrasound to confirm gestational age; signed informed consent form at least 24 hours in advance of procedure start time, and thorough review of patient history conducted by a licensed physician. Patients were fully informed that both abortion options include pain management, telehealth or in-person follow-up visits, and access to a 24-hour nurse advice service. While public and private insurance does not cover voluntary termination of pregnancy in the State of Michigan, at SWC, there was no difference in cost between first trimester surgical or medical abortion options.6 The primary difference between the abortion procedure types, besides the location in which the pregnancy tissue was passed, was the time spent within the clinic. For the medical abortion, patients left the clinic within two hours of their visit, whereas for the surgical abortions, patients were instructed that the process within the clinic could take up to six hours.
At the time of the study, SWC offered the first trimester surgical abortion to patients with a gestational age up to 12 weeks, 6 days, and the medical abortion to patients with a gestational age up to 10 weeks, 0 days.6 Performed by a licensed physician in an operating room, the physician used a series of rods to dilate the patient’s cervix in order to complete the surgical abortion; the pregnancy tissue was removed via vacuum aspiration.7 The medical abortion (“pill” or “at home” abortion) was initiated in the provider’s office and completed at the patient’s home. Using a series of medications prescribed by a licensed physician, patients took mifepristone (Mifeprex, 200 milligram dose) to block progesterone; then, 24 to 48 hours later, the patient administered four tablets of misoprostol (800 microgram dose) buccally or vaginally, passing the pregnancy tissue in the privacy of their home.6
2. Materials and Methods
2.1. Literature Review
A literature review on abortion care research since 2010 was conducted. The searches primarily focused on PubMed, with key terms including: abortion, access, Michigan, Midwest, independent providers, COVID-19, and pregnancy termination. National data published by the Centers for Disease Control and Prevention (CDC) and Guttmacher Institute contributed to the review; abortion statistics from The State of Michigan were utilized as well. The study protocol was determined to be non-human subject research and subsequently exempt from IRB approval. A research study request was submitted to all nine abortion clinics in Southeastern Michigan, and over a period of six months, only SWC agreed to take part in the study. A formal research proposal was submitted to and accepted by the Medical Director of SWC.
2.2. Data Collection and Ethics
With written and verbal permission from the Medical Director, the following documents from SWC were obtained from a secure, localized records database from 2019 and 2020 for data collection purposes only: post-procedure patient logs, mifepristone documentation logs, and physician documentation of abortion type by month. Retrospective, de-identified data regarding the count and type of first trimester abortions, performed January 1, 2019 through December 31, 2020, was collected. Data collection followed HIPAA confidentiality guidelines. The authors declare no conflict of interest. No funding was provided by any entities at any point during the duration of this study. All applicable ethical, clinical, and institutional guidelines for the collection and use of patient data were followed. Verbal and written consent for the use of relevant patient information was obtained during the initial patient appointment in compliance with HIPAA policy. Any reproduced materials in this paper were distributed under the terms of an open license and appeared in this paper as citations. Data supporting the findings of this study available from the corresponding author upon reasonable request.
2.3. Data Analysis
To quantify choice of abortion method between medical or surgical abortions, analysis examined the percentage of medical abortions relative to total first trimester abortions. A logistic regression time-period variable assessed for chronological trends over the 24-month period. Each calendar year was then divided into quartile periods of three consecutive months: Quarter 1 (Q1) represented abortions performed in January, February, and March; Quarter 2 (Q2) represented April, May, and June; Quarter 3 (Q3) represented July, August, and September; and Quarter 4 (Q4) represented October, November, and December. To account for any potential random seasonal fluctuations, the percentage of medical abortions for each quarter of 2020 was compared to the percentage of medical abortions from respective quarters of 2019 using a negative binomial statistical model. JMP software quantified the results.
3. Results
3.1. Month-to-Month Trend between 2019 to 2020 Based on Abortion Type
In 2019, there were 2,221 first trimester abortions (surgical =1,519, medical = 702). In 2020, there were 2,482 first trimester abortions (surgical =1,503, medical = 979). Statistical analysis between the total number of medical abortions in 2019 compared to 2020 revealed a significant increase in medical abortions (p-value = 0.00499). The logistic regression time-period analysis that accounted for individual months 1 through 24 (January 2019 through December 2020) resulted in a significant increase chronologically throughout the two years (p-value = 0.00824).
3.2. Quartile Comparison Based on Frequency of Medical Abortions
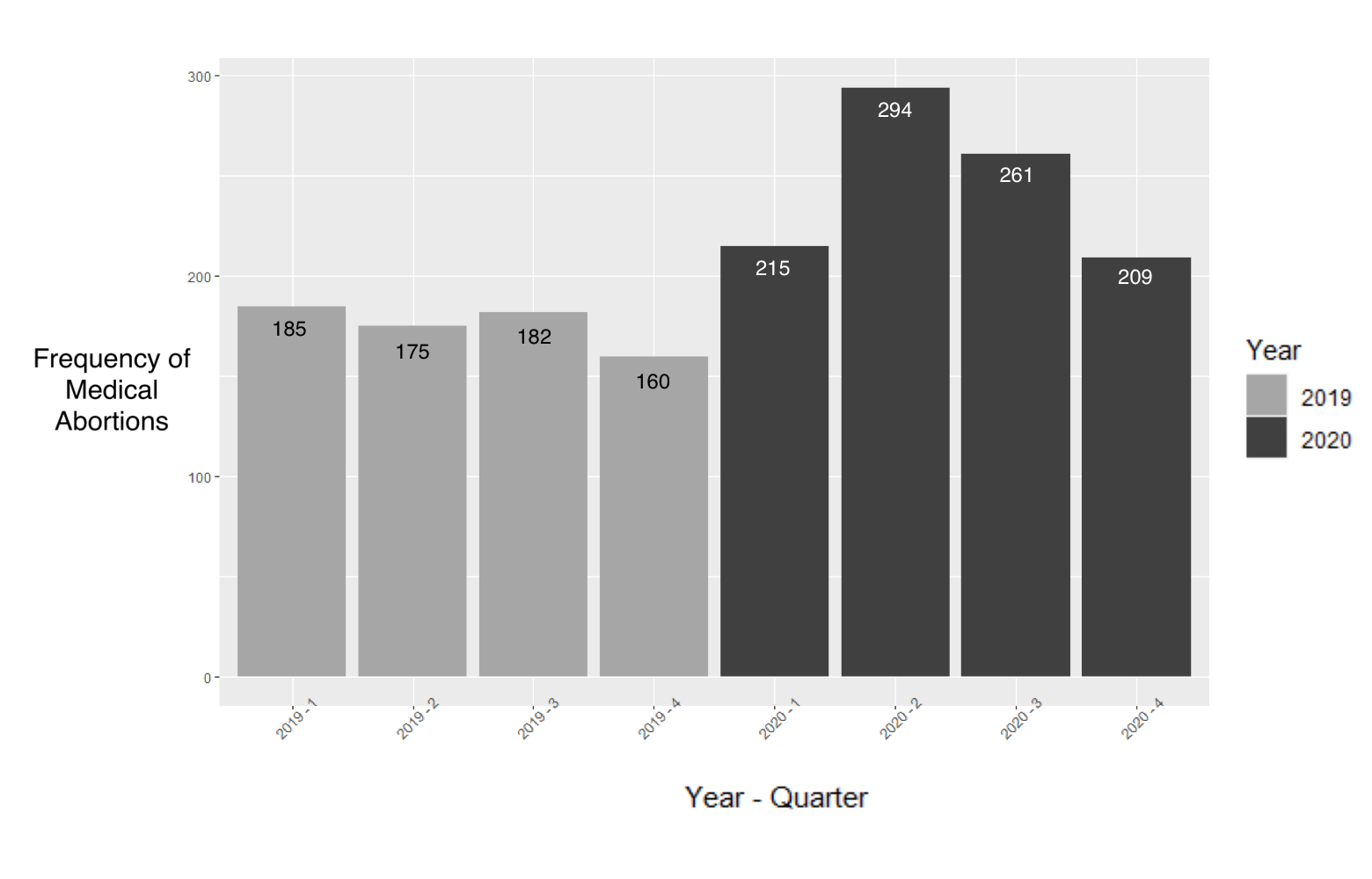
The frequency of medical abortions in 2019 and 2020, divided into quarters, is shown in Figure 1. In 2019, in Q1 to Q4, the frequency of medical abortions was 185, 175, 182, and 160, respectively. In 2020, in Q1 to Q4, the frequency of medical abortions was 215, 294, 261, and 209, respectively.

3.3. Quartile Percentages of Medical Abortions Compared to Total First Trimester Abortions
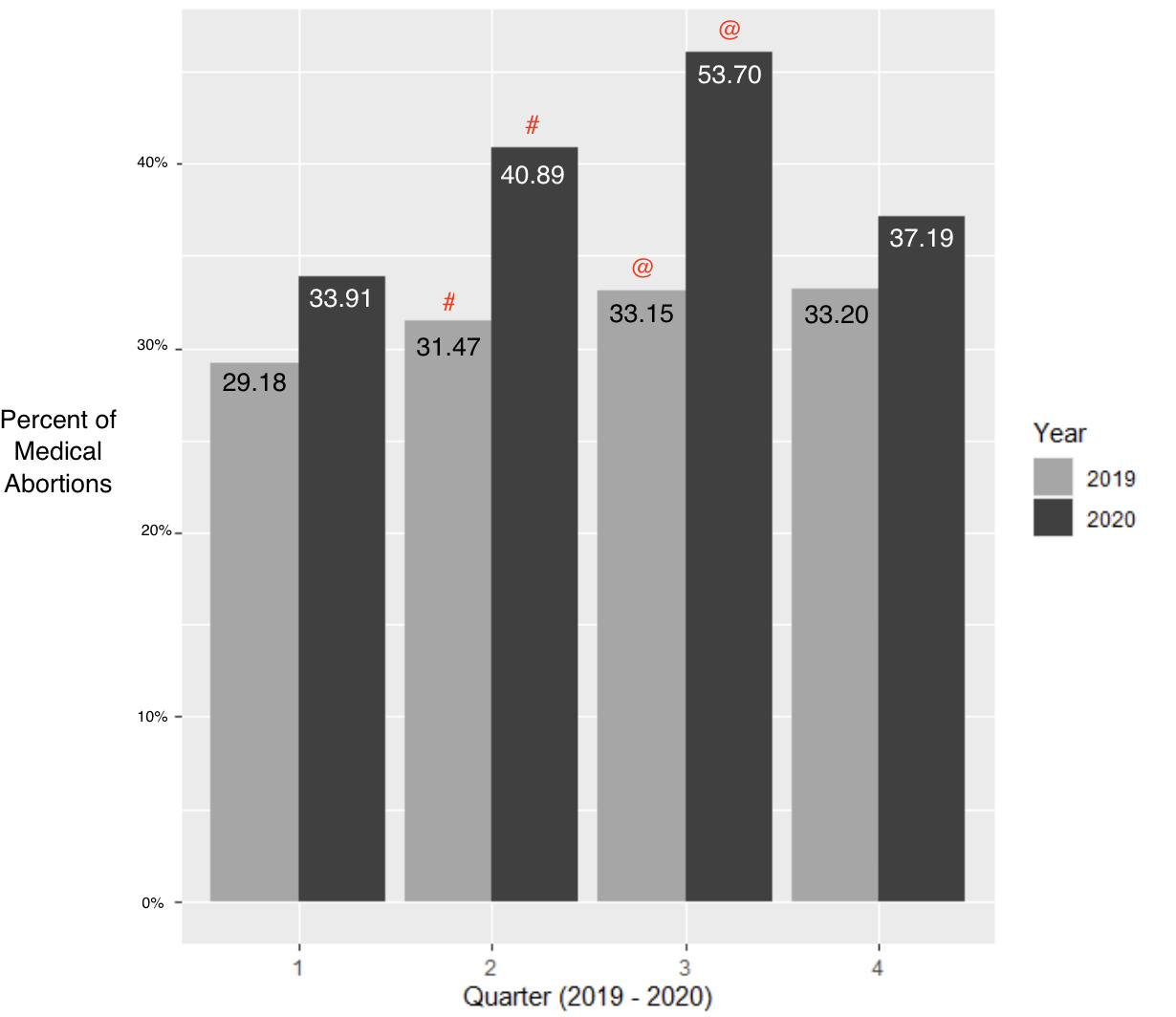
The percentage of medical abortions relative to the total number of first trimester abortions in 2019 and 2020, divided in quarters, is shown in Figure 2. In 2019, in Q1 to Q4, the percent of medical abortions was 29.18%, 31.47%, 33.15%, and 33.20%, respectively. In 2020, in Q1 to Q4, the percent of medical abortions was 33.91%, 40.89%, 53.70%, and 37.19%, respectively. In addition, analysis revealed the percentage difference between 2019 Q2 to 2020 Q2 and between 2019 Q3 and 2020 Q3 was statistically significant (p-values < 0.001). In comparing 2019 to 2020 in Q1, the 95% confidence interval (CI) was between -0.53% and 9.99% (p-value = 0.07968); in Q2, the CI was between 3.98% and 14.85% (p-value = 0.00068); in Q3, the CI was between 7.01% and 18.75% (p-value = 0.00001454); and in Q4, the CI was between -1.99% and 9.99% (p-value = 0.20030).

4. Discussion
4.1. Principal Findings
One healthcare clinic in Detroit, Michigan saw a statistically significant increase in the percentage of medical abortions relative to total first trimester abortions in the months following Michigan’s COVID-19 social distancing executive order in comparison to the same time period of the previous year. This increase returned to baseline by September 2020, three months after the expiration of the executive order. There was no significant difference in the percentage of medical abortions in the months prior to the enactment of the executive order.
4.2. Results
Statistically significant differences between 2019 and 2020 for Q2 and Q3 support the hypothesis that an increase in preference toward medical abortions over surgical abortions would be expected due to COVID-19 social distancing guidelines enacted on March 24, 2020. This was further supported by insignificant differences in 2019 and 2020 for Q1 and Q4, representing a return-to-baseline after the executive order expired on June 1, 2020.
4.3. Clinical Implications
In efforts to curtail the spread of the novel SARS-CoV-2 virus, many geographical regions entered a state of quarantine. In Michigan, a “stay-at-home” executive order was enacted on March 24, 2020 and lifted on June 1, 2020.4 If this government order were to impact patient choice for medical abortions as hypothesized, then medical abortion trends would reflect significant increases in medical abortions compared to surgical abortions in the months following March 24, 2020. Additionally, data should reflect a return-to-baseline after the executive order expired on June 1, 2020.4 Data analysis revealed trends that supported this hypothesis. As a result, implications could be reasonably drawn to assume that patients preferred medical abortions over surgical abortions during this period. Given the correspondence with the executive order, this is likely due to the shorter in-person clinic visit and increased physical privacy afforded by medical abortion methods. These findings, coupled with existing literature that prove the efficacy and safety of medical abortions,7–10 further supports ongoing efforts to establish medication-induced abortions as a legitimate option for first trimester voluntary termination of pregnancy.
This data could be utilized to not only further understand the patient’s choice of abortion, but also to expand abortion access. During the pandemic, healthcare providers modified services to minimize the time necessary during in-person visits, while increasing availability of telemedicine visits.11 Patients have been increasingly willing to receive telehealth services, with nearly 62% of patients from a consumer study stating that they would be willing to use virtual care in the future.12 Expanding abortion access via telemedicine with the medical abortion option may be more feasible that surgical abortions in rural and underdeveloped communities, thus avoiding outpatient surgical facility requirements, difficulties accessing necessary equipment for the procedure, reliable electricity and staffing, among other concerns.13
4.4. Research Implications
Nationwide research on medical abortion trends during each state’s respective “stay-at-home” order is needed. Additional research should include qualitative studies in order to evaluate trends in patient preference toward pregnancy termination methods during the SARS-CoV-2 pandemic.
4.5. Strengths and Limitations
This has contributed several novel perspectives regarding first trimester abortion trends during the SARS-CoV-2 pandemic. The increase in percentage of medical abortions over total first trimester abortions at a high volume independent clinic in Detroit differs from a previous publication based in Southern California.3 With each study displaying different trends, statistical measures, and pre- and post-abortion procedures, the authors of this publication seek to provide valuable insight, highlighting the difference in human response across the country during a pandemic. In addition, this research utilized a novel approach to account for potential seasonal fluctuations in abortion trends by directly comparing each quarter from 2020 to the respective quarter from 2019.
Several limitations were uncovered during data analysis. The largest limitation was the lack of participation from other clinics in the Southeastern Michigan area. Because data was compiled from only one of the nine abortion clinics, the sample population could be skewed. Further research should be conducted to determine if similar trends were observed in clinics across the nation. Qualitative research should be employed to assess patient perspectives on the process of choosing between a surgical or medical abortion. Additional research could focus on areas that have allowed completely virtual medical abortion visits to determine factors such as patient satisfaction with care and patient compliance with instructions. Another limitation dealt with unequal division of gestational age between medical and surgical abortions. The sample of surgical abortions were performed up to 12 weeks, 6 days; thus, the data does not account for those not eligible for the medical abortion, as they were over the 10 week, 0 day limit. An additional limitation included the lack of accounting for the preference/desire for a medical abortion. Patients may have preferred a medical abortion but did not realize that they were pregnant until further into their gestation, was unable to afford an abortion at an earlier appointment, was unsure of their decision, or was delaying care due to COVID-19. The last limitation addressed not accounting for the preference/desire for a surgical abortion. Patients may have preferred a surgical abortion but did not have a required driver necessary to receive sedative medication.
Author Contributions
The two primary authors contributed equally to the work, with support from J Dennis.
Funding
This research did not receive any specific grant(s) from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Interest
None.
Acknowledgements
We wish to extend special thanks to the members of SWC: SAM, Executive Director, for her support; Dr. RJE, Medical Director, for his assistance and oversight; and to the staff, for their dedication to providing compassionate care. An additional warm thanks to Dr. MT and Dr. FL of Michigan State University College of Human Medicine for their support and guidance.